

The effect of timing and graft dysfunction on survival and cardiac allograft vasculopathy in antibody-mediated rejection
- PMID: 27423693
- PMCID: PMC5662939
- DOI: 10.1016/j.healun.2016.04.007
The effect of timing and graft dysfunction on survival and cardiac allograft vasculopathy in antibody-mediated rejection
Abstract
Background: Antibody-mediated rejection (AMR) has been associated with increased death and cardiac allograft vasculopathy (CAV). Early studies suggested that late AMR was rarely associated with graft dysfunction, whereas recent reports have demonstrated an association with increased mortality. We investigated the timing of AMR and its association with graft dysfunction, death, and CAV.
Methods: This retrospective cohort study identified all adult orthotopic heart transplant (OHT) recipients (N = 689) at Columbia University Medical Center from 2004 to 2013. There were 68 primary cases of AMR, which were stratified by early (< 1 year post-OHT) or late (> 1 year post-OHT) AMR. Kaplan-Meier survival analysis and modeling was performed with multivariable logistic regression and Cox proportional hazards regression.
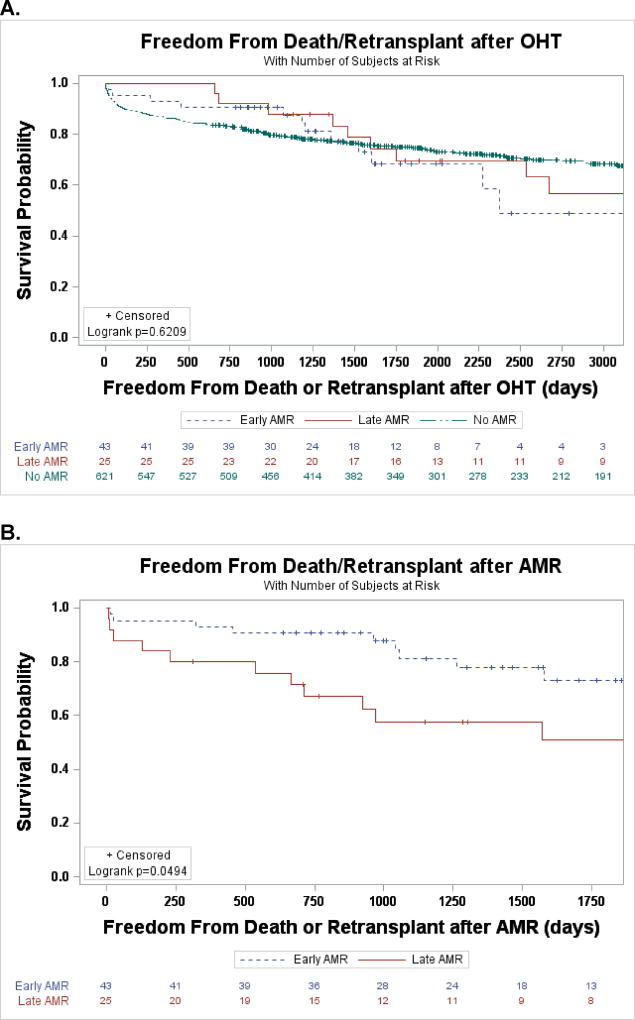
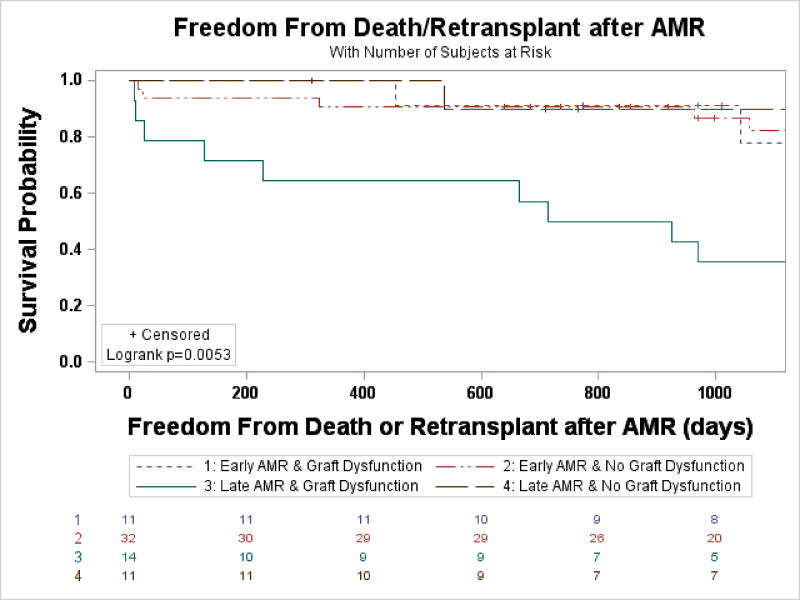
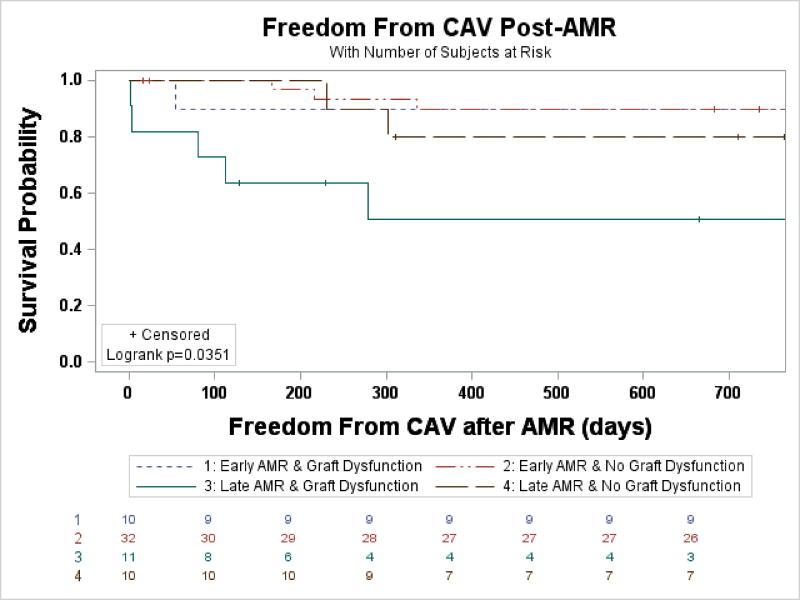
Results: From January 1, 2004, through October 1, 2015, early AMR (median 23 days post-OHT) occurred in 43 patients and late AMR (median 1,084 days post-OHT) occurred in 25. Graft dysfunction was less common with early compared with late AMR (25.6% vs 56%, p = 0.01). Patients with late AMR had decreased post-AMR survival compared with early AMR (1 year: 80% vs 93%, 5 years: 51% vs 73%, p < 0.05). When stratified by graft dysfunction, only those with late AMR and graft dysfunction had worse survival (30 days: 79%, 1 year: 64%, 5 years: 36%; p < 0.006). The association remained irrespective of age, sex, donor-specific antibodies, left ventricular assist device use, reason for OHT, and recovery of graft function. Similarly, those with late AMR and graft dysfunction had accelerated development of de novo CAV (50% at 1 year; hazard ratio, 5.42; p = 0.009), whereas all other groups were all similar to the general transplant population.
Conclusions: Late AMR is frequently associated with graft dysfunction. When graft dysfunction is present in late AMR, there is an early and sustained increased risk of death and rapid development of de novo CAV despite aggressive treatment.
Keywords: antibody-mediated rejection; cardiac allograft vasculopathy; donor specific antibodies; graft dysfunction; mortality.
Copyright © 2016 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Early and late AMR in heart transplantation-Distinct entities?J Heart Lung Transplant. 2016 Sep;35(9):1055-6. doi: 10.1016/j.healun.2016.07.005. Epub 2016 Jul 16. J Heart Lung Transplant. 2016. PMID: 27578597 No abstract available.
References
-
- Lund LH, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-second Official Adult Heart Transplantation Report-2015; Focus Theme: Early Graft Failure. J Heart Lung Transplant. 2015;34:1244–54. - PubMed
-
- Takemoto SK, Zeevi A, Feng S, et al. National conference to assess antibody-mediated rejection in solid organ transplantation. Am J Transplant. 2004;4:1033–41. - PubMed
-
- Michaels PJ, Espejo ML, Kobashigawa J, et al. Humoral rejection in cardiac transplantation: risk factors, hemodynamic consequences and relationship to transplant coronary artery disease. J Heart Lung Transplant. 2003;22:58–69. - PubMed
-
- Reed EF, Demetris AJ, Hammond E, et al. Acute antibody-mediated rejection of cardiac transplants. J Heart Lung Transplant. 2006;25:153–9. - PubMed
-
- Kfoury AG, Renlund DG, Snow GL, et al. A clinical correlation study of severity of antibody-mediated rejection and cardiovascular mortality in heart transplantation. The Journal of heart and lung transplantation: the official publication of the International Society for Heart Transplantation. 2009;28:51–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
