

Integrating conventional and antibody-based targeted anticancer treatment into immunotherapy
- PMID: 27425593
- PMCID: PMC5243926
- DOI: 10.1038/onc.2016.231
Integrating conventional and antibody-based targeted anticancer treatment into immunotherapy
Abstract
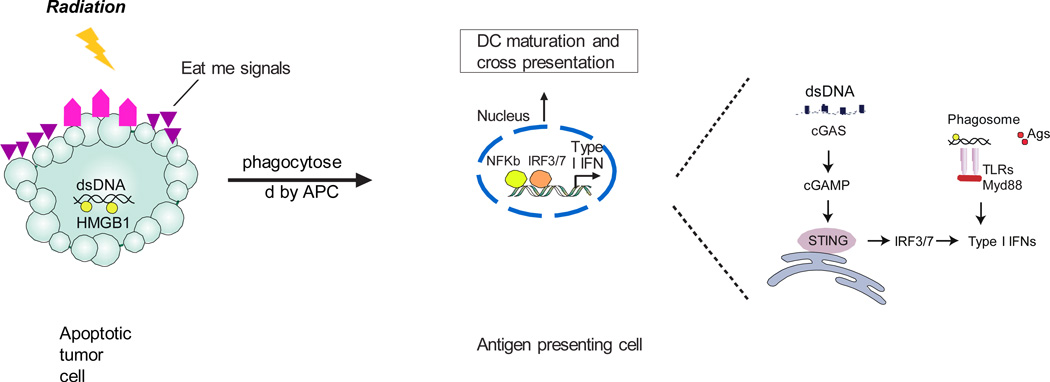
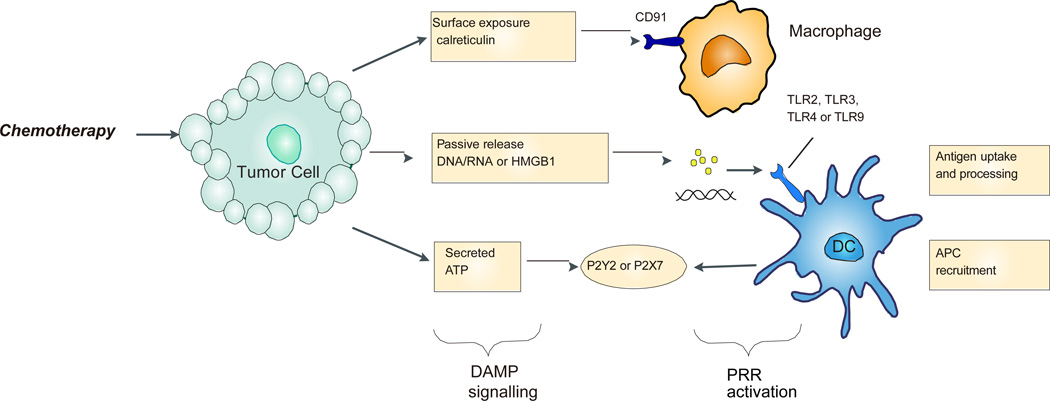
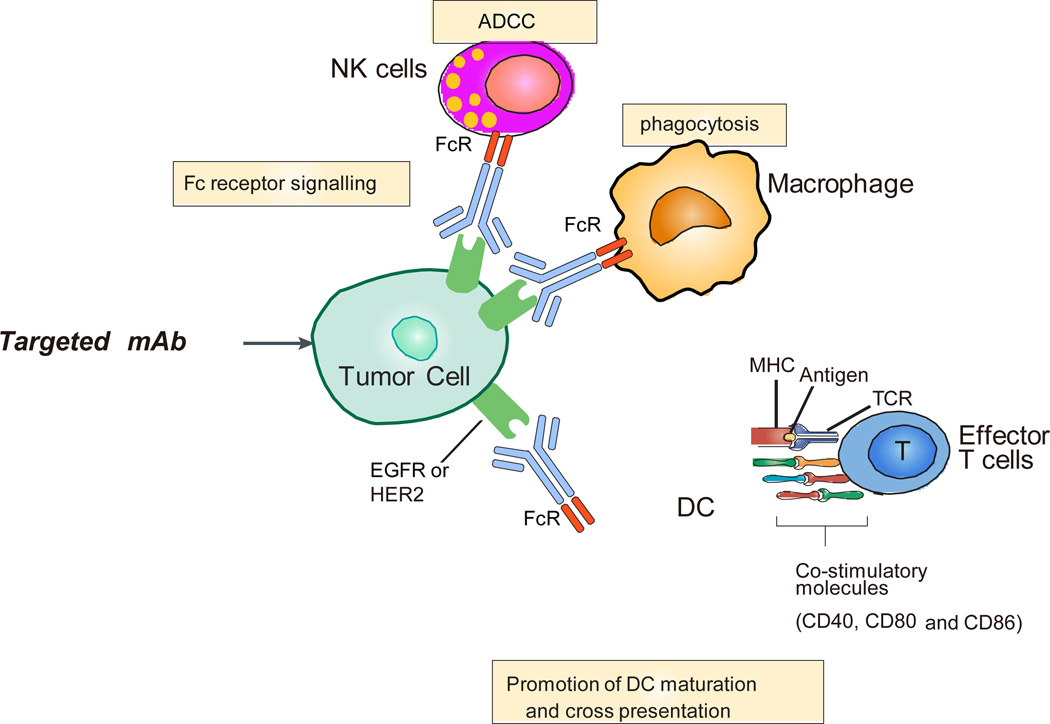
In advanced cancer, current conventional therapies or immunotherapies cannot eradicate all tumor cells for most patients. Integration of these two treatments for synergistic effects could eradicate more tumor cells and increase the overall survival rates. However, since how conventional treatments impact on immune system remains unclear, proper integration is still a challenge. Intensive chemo/radiotherapy may impair ongoing immune responses, while lower intensity of therapy might not kill enough tumor cells, both leading to tumor relapse. Current understanding of mechanisms of resistance to conventional and targeted cancer therapies has focused on cell intrinsic pathways that trigger DNA damage/repair or signaling pathways related to cell growth. Recent reports show that host T cells properly primed against tumor-specific antigens after conventional treatment, which can integrate with direct cytotoxic effects induced by radiation or chemotherapy to profoundly control tumors. Following cytotoxic anticancer treatment, tumor-derived DAMPs (damage-associated molecular patterns) can be sensed by innate cells, which drives type I interferon production for cross-priming of CD8+ T cells. Some types and protocols of chemotherapy or radiation can increase tumor-infiltrating lymphocytes that overcome resistance to immunotherapy. As such, a deeper understanding of the immune mechanisms of conventional and targeted cancer therapies will lead toward novel combinatorial anticancer strategies with improved clinical benefit.
Figures
References
-
- Waun Ki Hong RCBJ, Hait William N, Kufe Donald W, Pollock Raphael E, Weichselbaum Ralph R, Holland James F, Frei Emil., III . Cancer Medicine. 8th. Shelton, Connecticut: People’s Medical Publishing House –USA; 2010.
-
- Larkin J, Hodi FS, Wolchok JD. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med. 2015;373(13):1270–1271. - PubMed
-
- Kelland L. The resurgence of platinum-based cancer chemotherapy. Nat Rev Cancer. 2007;7(8):573–584. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
