

Ganglionated plexi and ligament of Marshall ablation reduces atrial vulnerability and causes stellate ganglion remodeling in ambulatory dogs
- PMID: 27426436
- PMCID: PMC5149413
- DOI: 10.1016/j.hrthm.2016.07.014
Ganglionated plexi and ligament of Marshall ablation reduces atrial vulnerability and causes stellate ganglion remodeling in ambulatory dogs
Abstract
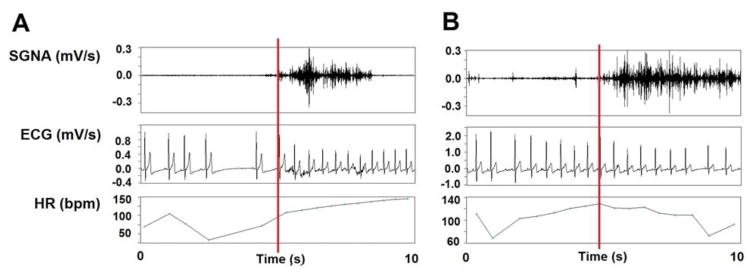
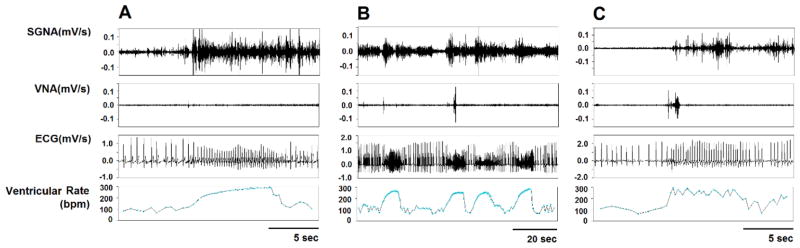
Background: Simultaneous activation of the stellate ganglion (SG), the ligament of Marshall (LOM), and the ganglionated plexi often precedes the onset of paroxysmal atrial tachyarrhythmia (PAT).
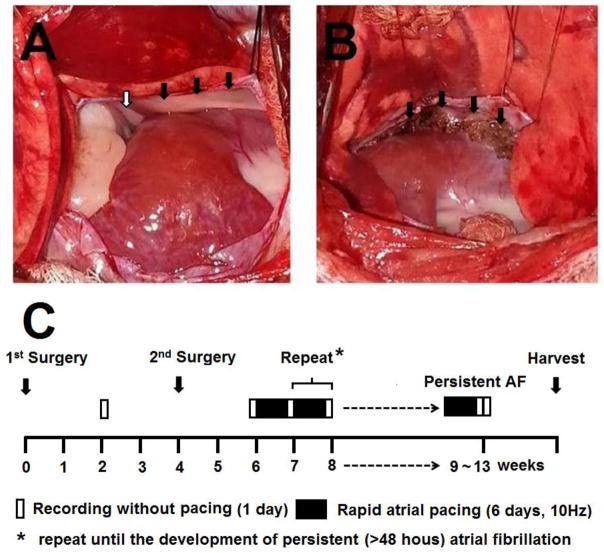
Objective: The purpose of this study was to test the hypothesis that ablation of the LOM and the superior left ganglionated plexi (SLGP) reduces atrial vulnerability and results in remodeling of the SG.
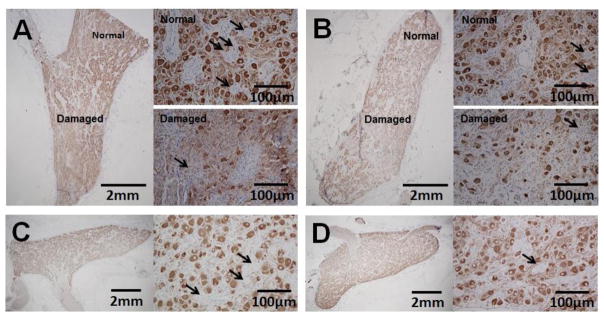
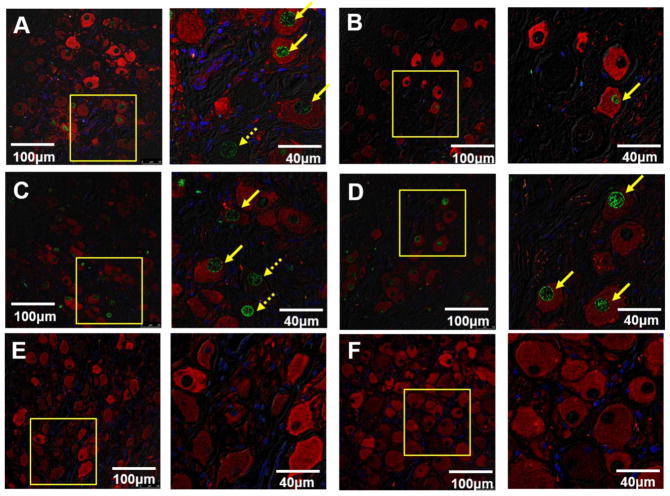
Methods: Nerve activity was correlated to PAT and ventricular rate (VR) at baseline, after ablation of the LOM and SLGP, and after atrial fibrillation. Neuronal cell death was assessed with tyrosine hydroxylase and terminal deoxynucleotidyl transferase dUTP nick end label (TUNEL) staining.
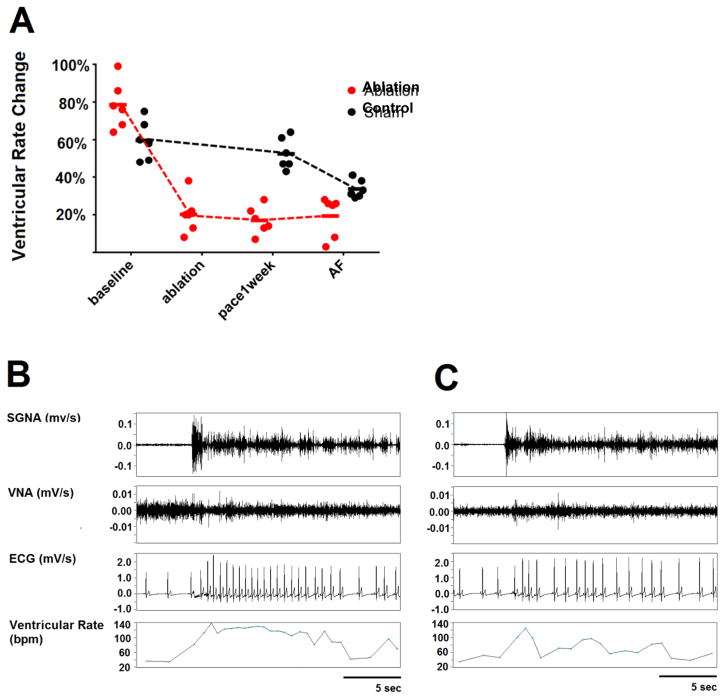
Results: There were 4 ± 2 PAT episodes per day in controls. None were observed in the ablation group, even though SG nerve activity and VR increased from 2.2 µV (95% confidence interval [CI] 1.2-3.3 µV) and 80 bpm (95% CI 68-92 bpm) at baseline, to 3.0 µV (95% CI 2.6-3.4 µV, P = .046) and 90 bpm (95% CI 75-108 bpm, P = .026) after ablation, and to 3.1 µV (95% CI 1.7-4.5 µV, P = .116) and 95 bpm (95% CI 79-110 bpm, P = .075) after atrial fibrillation. There was an increase in tyrosine hydroxylase-negative cells in the ablation group and 19.7% (95% CI 8.6%-30.8%) TUNEL-positive staining in both the left and right SG. None were observed in the control group.
Conclusion: LOM and SLGP ablation caused left SG remodeling and cell death. There was reduced correlation of the VR response and PAT to SG nerve activity. These findings support the importance of SLGP and LOM in atrial arrhythmogenesis.
Keywords: Ablation; Atrial fibrillation; Ligament of Marshall; Superior left ganglion plexi.
Copyright © 2016 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Armour JA. Cardiac neuronal hierarchy in health and disease. AmJPhysiol RegulIntegrComp Physiol. 2004;287:R262–R271. - PubMed
-
- Hou Y, Zhou Q, Po SS. Neuromodulation for cardiac arrhythmia. Heart Rhythm Feb. 2016;13:584–592. - PubMed
-
- Makino M, Inoue S, Matsuyama TA, Ogawa G, Sakai T, Kobayashi Y, Katagiri T, Ota H. Diverse myocardial extension and autonomic innervation on ligament of Marshall in humans. J Cardiovasc Electrophysiol Jun. 2006;17:594–599. - PubMed
-
- Hou Y, Scherlag BJ, Lin J, Zhang Y, Lu Z, Truong K, Patterson E, Lazzara R, Jackman WM, Po SS. Ganglionated plexi modulate extrinsic cardiac autonomic nerve input: effects on sinus rate, atrioventricular conduction, refractoriness, and inducibility of atrial fibrillation. JAmCollCardiol. 2007;50:61–68. - PubMed
-
- Lin J, Scherlag BJ, Niu G, Lu Z, Patterson E, Liu S, Lazzara R, Jackman WM, Po SS. Autonomic elements within the ligament of Marshall and inferior left ganglionated plexus mediate functions of the atrial neural network. J Cardiovasc Electrophysiol Mar. 2009;20:318–324. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
