

AIRE-Deficient Patients Harbor Unique High-Affinity Disease-Ameliorating Autoantibodies
- PMID: 27426947
- PMCID: PMC4967814
- DOI: 10.1016/j.cell.2016.06.024
AIRE-Deficient Patients Harbor Unique High-Affinity Disease-Ameliorating Autoantibodies
Abstract
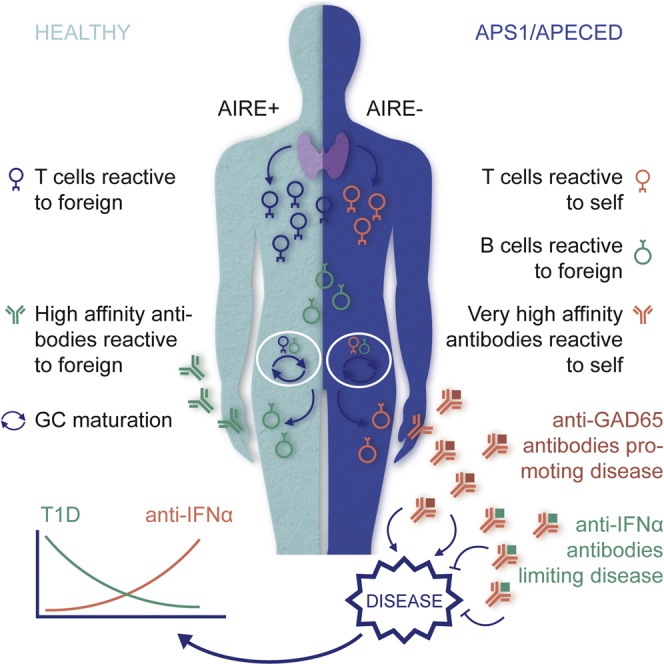
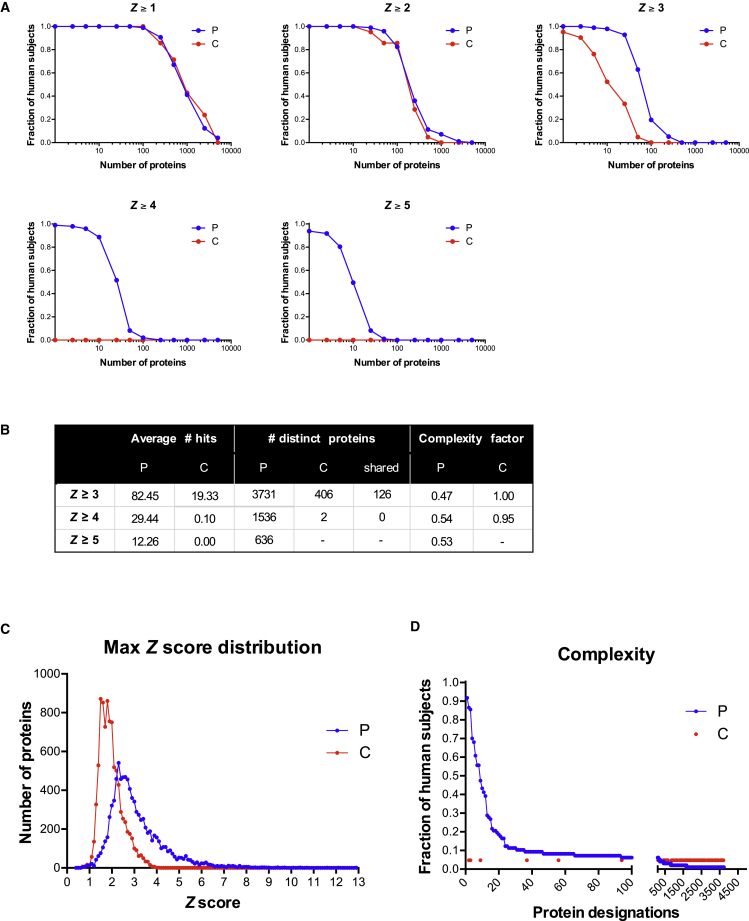
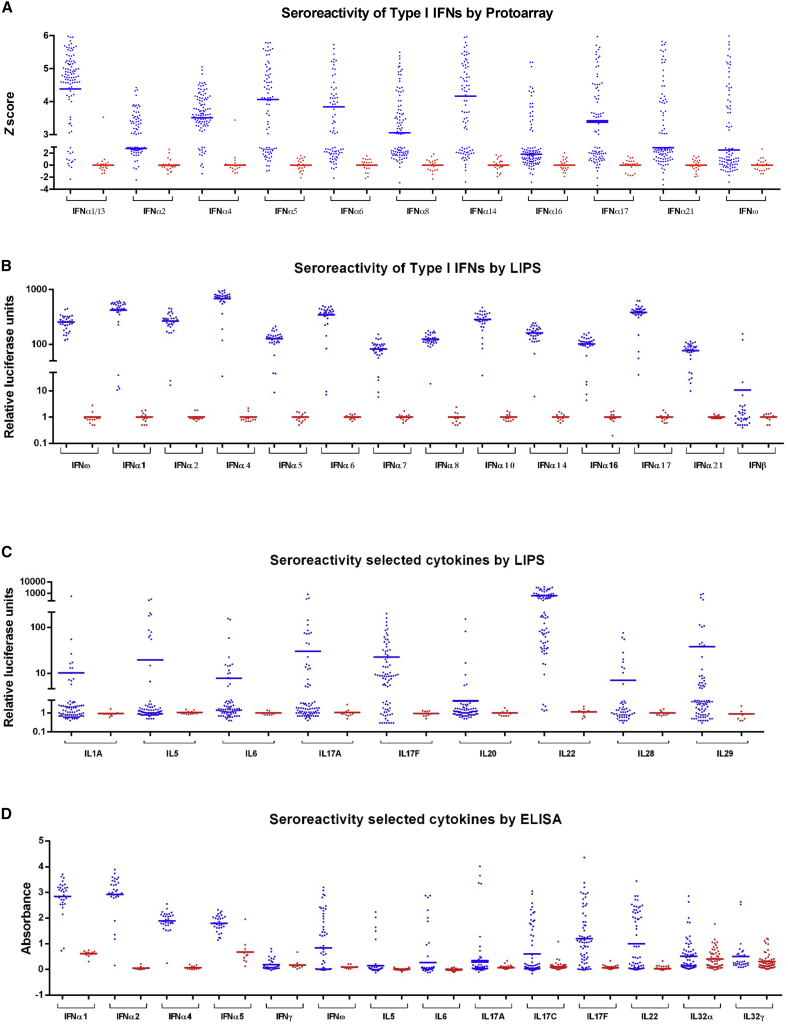
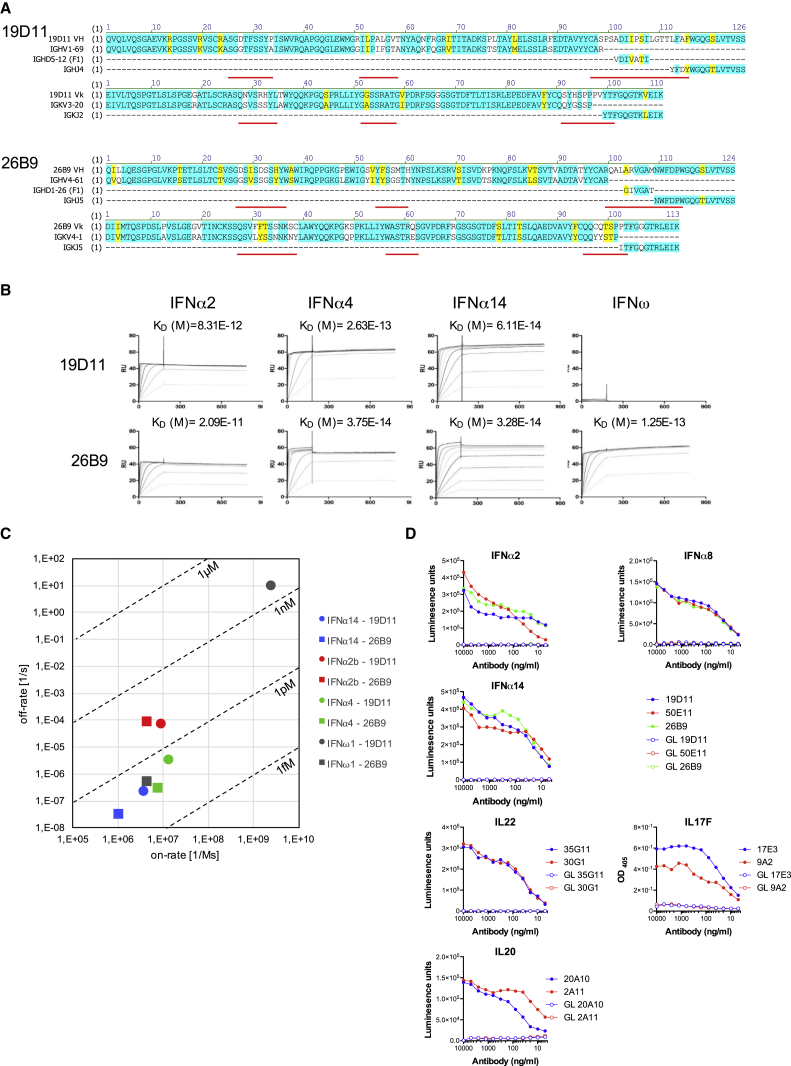
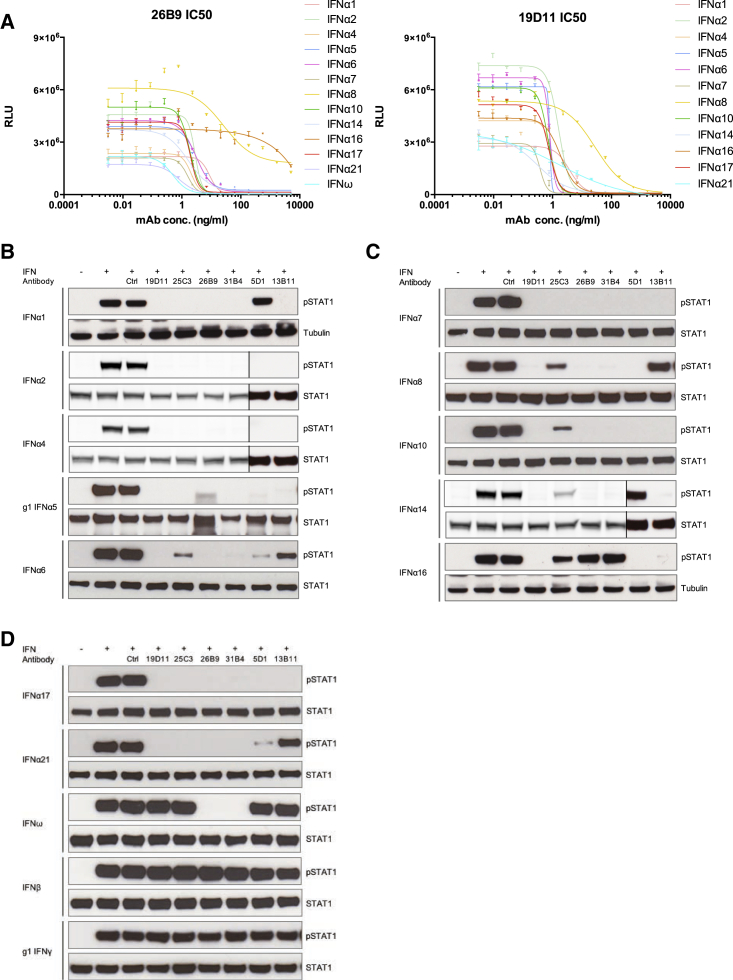
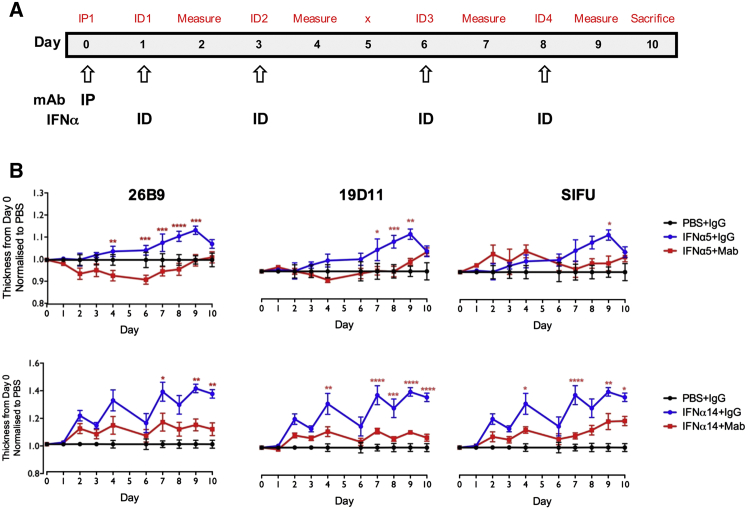
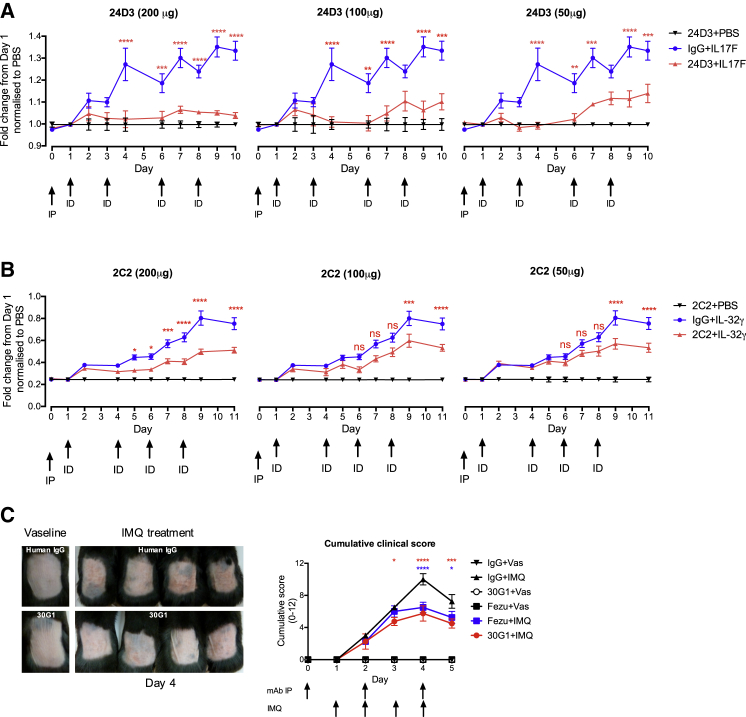
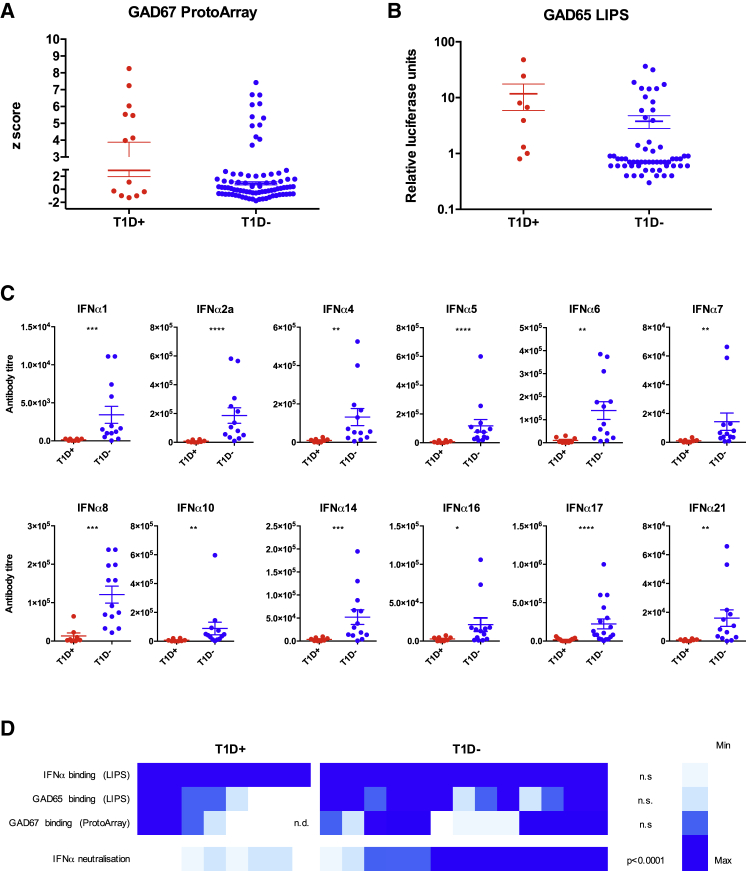
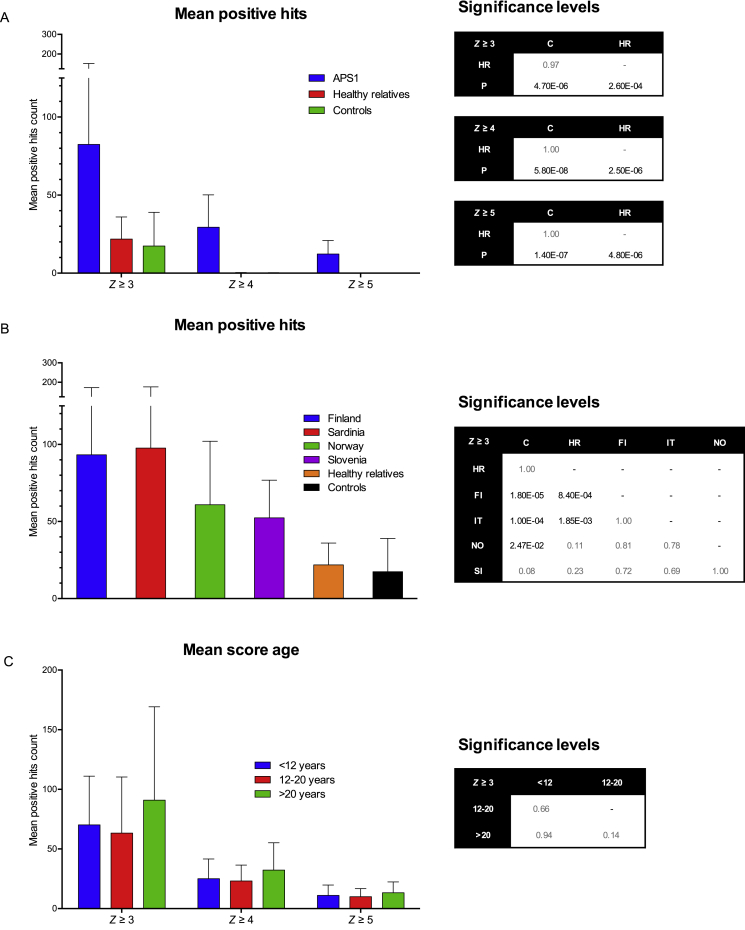
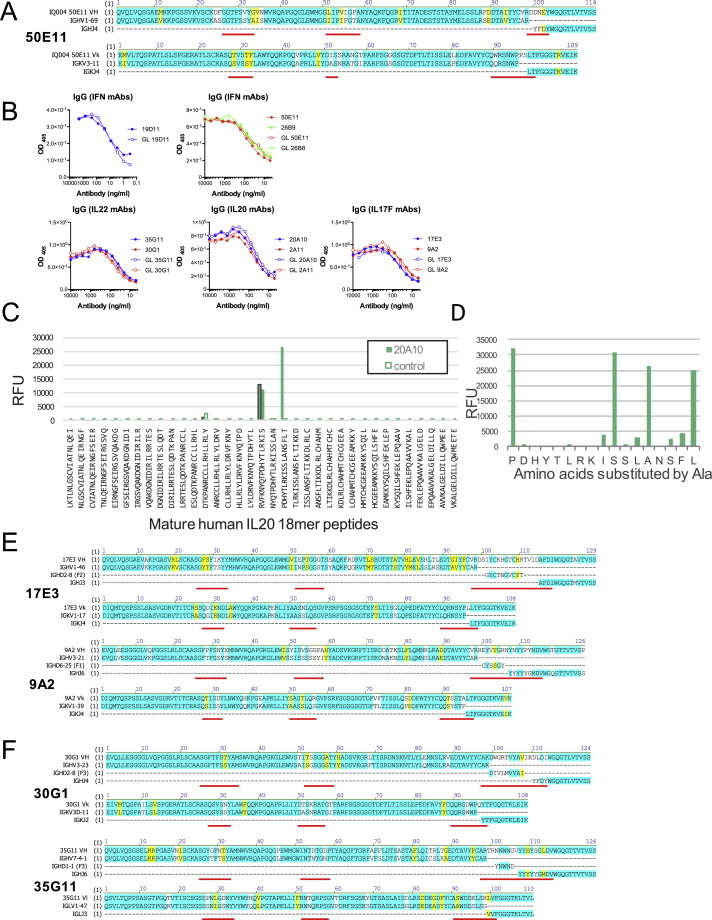
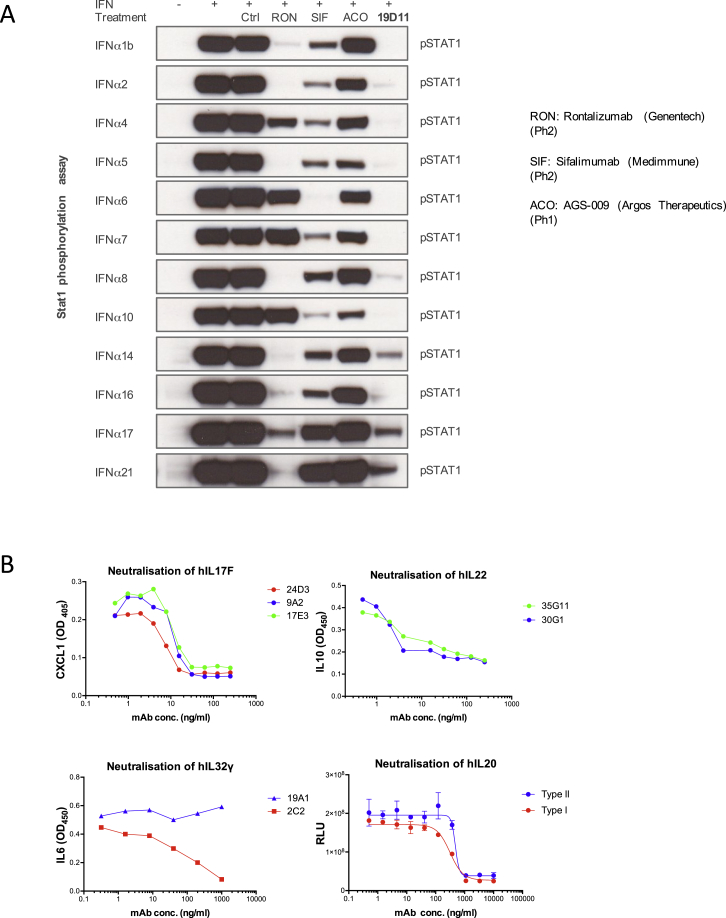
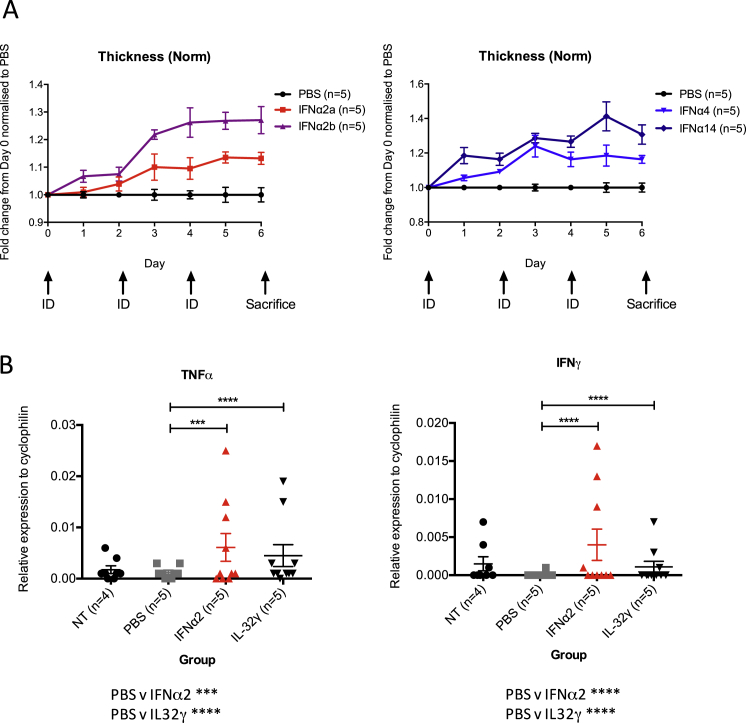
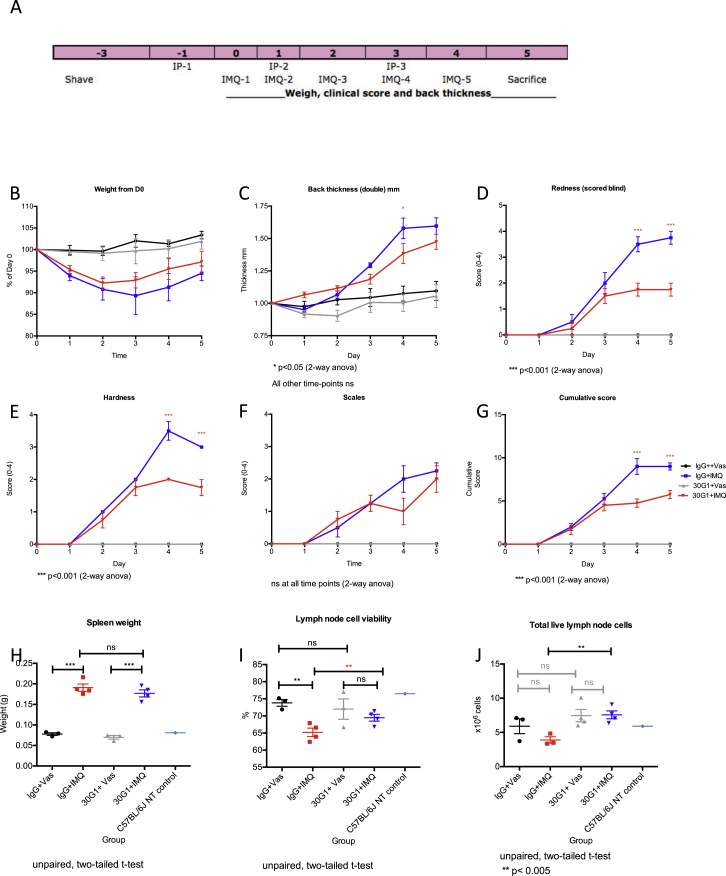
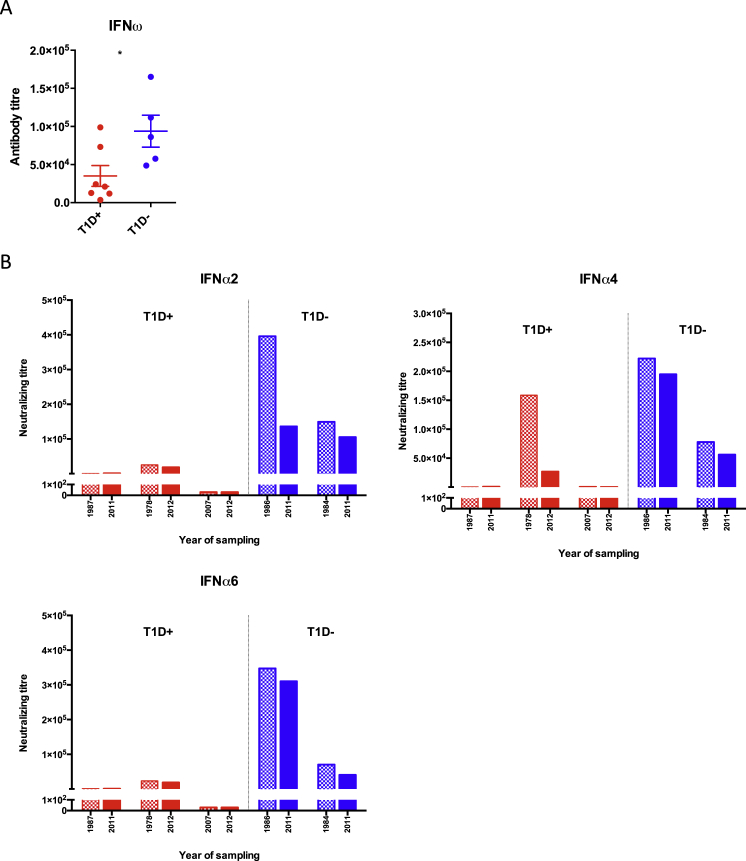
APS1/APECED patients are defined by defects in the autoimmune regulator (AIRE) that mediates central T cell tolerance to many self-antigens. AIRE deficiency also affects B cell tolerance, but this is incompletely understood. Here we show that most APS1/APECED patients displayed B cell autoreactivity toward unique sets of approximately 100 self-proteins. Thereby, autoantibodies from 81 patients collectively detected many thousands of human proteins. The loss of B cell tolerance seemingly occurred during antibody affinity maturation, an obligatorily T cell-dependent step. Consistent with this, many APS1/APECED patients harbored extremely high-affinity, neutralizing autoantibodies, particularly against specific cytokines. Such antibodies were biologically active in vitro and in vivo, and those neutralizing type I interferons (IFNs) showed a striking inverse correlation with type I diabetes, not shown by other anti-cytokine antibodies. Thus, naturally occurring human autoantibodies may actively limit disease and be of therapeutic utility.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
In Praise of Descriptive Science: A Breath of Fresh AIRE.Cell. 2016 Jul 28;166(3):530-531. doi: 10.1016/j.cell.2016.07.018. Cell. 2016. PMID: 27471960 Free PMC article.
-
Diabetes: Natural autoantibodies protect against T1DM.Nat Rev Endocrinol. 2016 Oct;12(10):560. doi: 10.1038/nrendo.2016.130. Epub 2016 Aug 5. Nat Rev Endocrinol. 2016. PMID: 27494388 No abstract available.
-
Autoimmunity: Autoantibodies with a silver lining?Nat Rev Immunol. 2016 Sep;16(9):536. doi: 10.1038/nri.2016.96. Epub 2016 Aug 16. Nat Rev Immunol. 2016. PMID: 27526641 No abstract available.
-
Comment on 'AIRE-deficient patients harbor unique high-affinity disease-ameliorating autoantibodies'.Elife. 2019 Jun 27;8:e43578. doi: 10.7554/eLife.43578. Elife. 2019. PMID: 31244471 Free PMC article.
References
-
- Ambrosi A., Espinosa A., Wahren-Herlenius M. IL-17: a new actor in IFN-driven systemic autoimmune diseases. Eur. J. Immunol. 2012;42:2274–2284. - PubMed
-
- Bennett C.L., Christie J., Ramsdell F., Brunkow M.E., Ferguson P.J., Whitesell L., Kelly T.E., Saulsbury F.T., Chance P.F., Ochs H.D. The immune dysregulation, polyendocrinopathy, enteropathy, X-linked syndrome (IPEX) is caused by mutations of FOXP3. Nat. Genet. 2001;27:20–21. - PubMed
-
- Brink R. The imperfect control of self-reactive germinal center B cells. Curr. Opin. Immunol. 2014;28:97–101. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
