

Fast track program in liver resection: a PRISMA-compliant systematic review and meta-analysis
- PMID: 27428206
- PMCID: PMC4956800
- DOI: 10.1097/MD.0000000000004154
Fast track program in liver resection: a PRISMA-compliant systematic review and meta-analysis
Abstract
Background: FT program (FT) is a multimodal approach used to enhance postoperative rehabilitation and accelerate recovery. It was 1st described in open heart surgery, then modified and applied successfully in colorectal surgery. FT program was described in liver resection for the 1st time in 2008. Although the program has become widely accepted, it has not yet been considered the standard of care in liver surgery.
Objectives: we performed this systematic review and meta-analysis to evaluate the impact of using the FT program compared to the traditional care (TC), on the main clinical and surgical outcomes for patients who underwent elective liver resection.
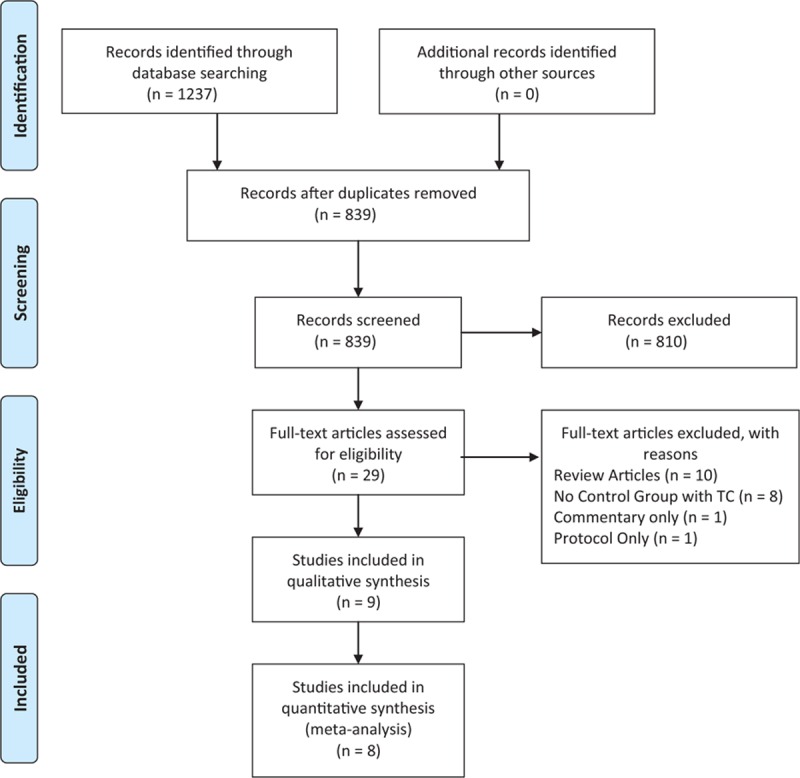
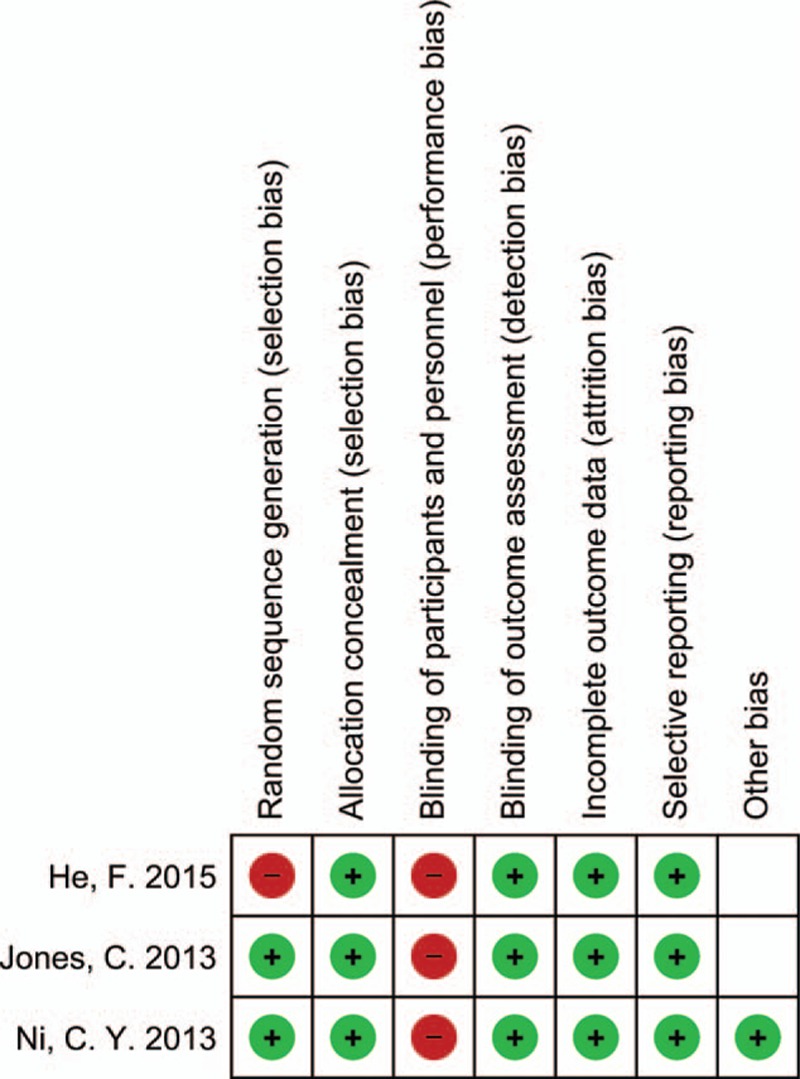
Methods: PubMed/Medline, Scopus, and Cochran databases were searched to identify eligible articles that compared FT with TC in elective liver resection to be included in this study. Subgroup meta-analysis between laparoscopic and open surgical approaches to liver resection was also conducted. Quality assessment was performed for all the included studies. Odds ratios (ORs) and mean differences (MDs) were considered as a summary measure of evaluating the association in this meta-analysis for dichotomous and continuous data, respectively. A 95% confidence interval (CI) was reported for both measures. I was used to assess the heterogeneity across studies.
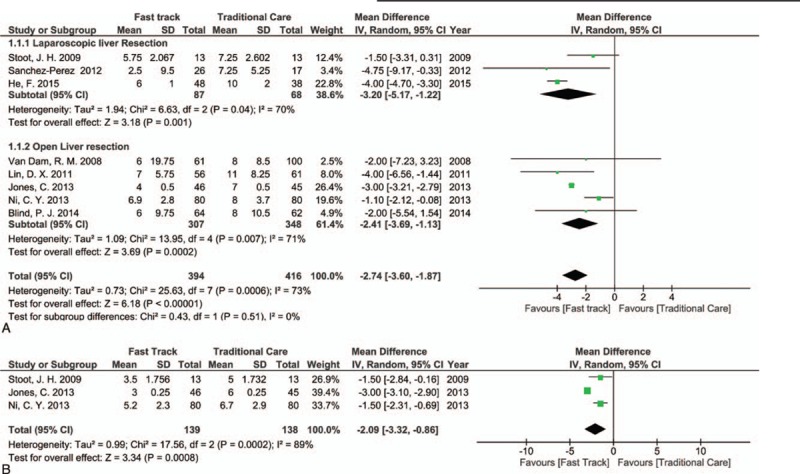
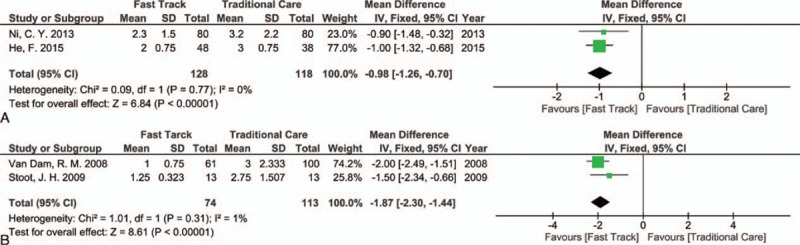
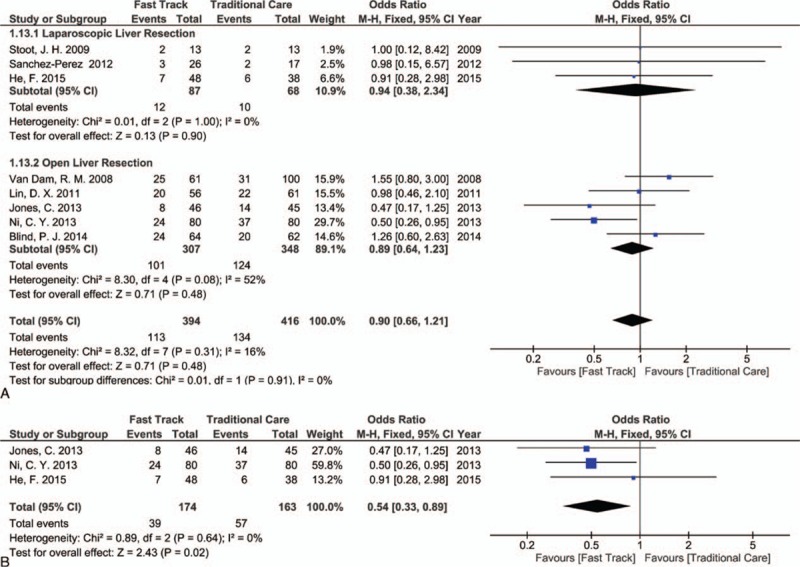
Results: From 2008 to 2015, 3 randomized controlled trials (RCTs) and 5 cohort studies were identified, including 394 and 416 patients in the FT and TC groups, respectively. The length of hospital stay (LoS) was markedly shortened in both the open and laparoscopic approaches within the FT program (P < 0.00001). The reduced LoS was accompanied by accelerated functional recovery (P = 0.0008) and decreased hospital costs, with no increase in readmission, morbidity, or mortality rates. Moreover, significant results were found within the FT group such as reduced operative time (P = 0.03), lower intensive care unit admission rate (P < 0.00001), early bowel opening (P ≤ 0.00001), and rapid normal diet restoration (P ≤ 0.00001).
Conclusion: FT program is safe, feasible, and can be applied successfully in liver resection. Future RCTs on controversial issues such as multimodal analgesia and adherence rate are needed. Specific FT guidelines should be developed for liver resection.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures

References
-
- van Dam RM, Hendry PO, Coolsen MM, et al. Initial experience with a multimodal enhanced recovery programme in patients undergoing liver resection. Br J Surg 2008; 95:969–975. - PubMed
-
- Krohn BG, Kay JH, Mendez MA, et al. Rapid sustained recovery after cardiac operations. J Thorac Cardiovasc Surg 1990; 100:194–197. - PubMed
-
- Engelman RM, Rousou JA, Flack JE, et al. Fast-track recovery of the coronary bypass patient. Ann Thorac Surg 1994; 58:1742–1746. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
