

Correlations of clinical, neuroimaging, and electrophysiological features in Hirayama disease
- PMID: 27428223
- PMCID: PMC4956817
- DOI: 10.1097/MD.0000000000004210
Correlations of clinical, neuroimaging, and electrophysiological features in Hirayama disease
Abstract
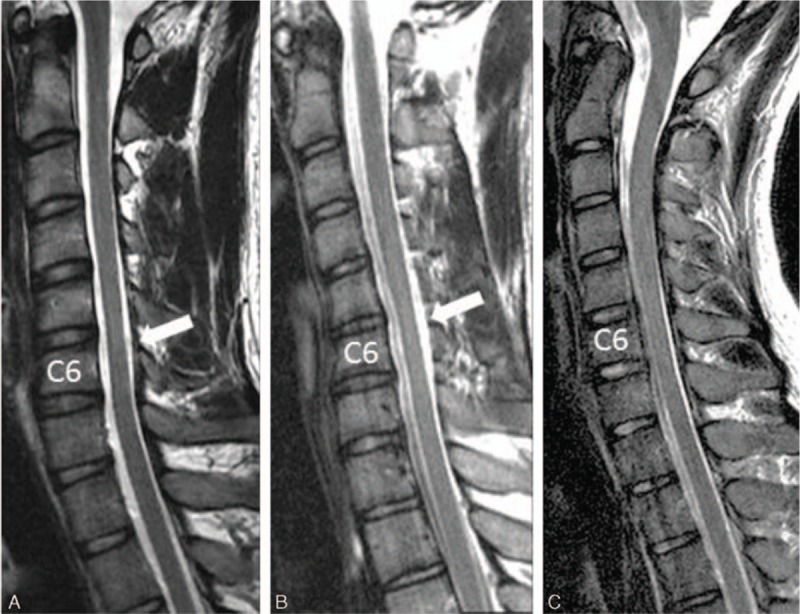
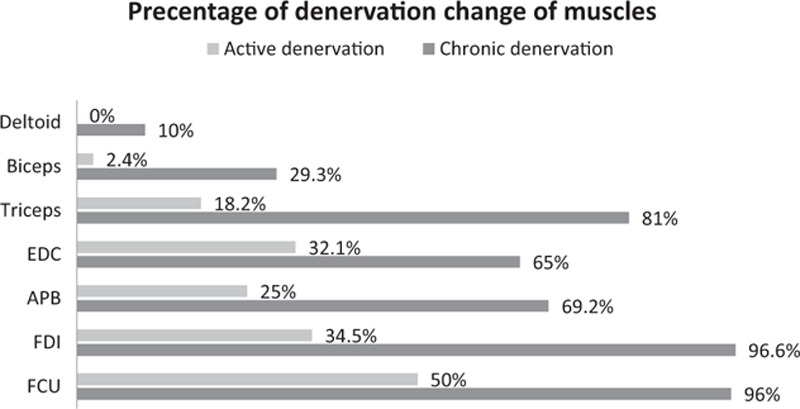
Hirayama disease (HD) is characterized by development of asymmetric forearm muscle atrophy during adolescence with or without focal cervical spinal cord atrophy. The purpose of this study is to assess the correlation of clinical symptoms, disease progression, and electrophysiological findings with cervical spine magnetic resonance imaging (MRI) findings.The medical records, cervical spine MRIs, and electrophysiological findings of 44 HD patients were retrospectively reviewed and analyzed.Denervation changes in any single C5 to C7 root-innervated muscle (deltoid, biceps, triceps, or extensor digitorum communis) occurred more frequently in the 25 patients with cord atrophy than the 19 patients without cord atrophy (88% vs 53%, P = 0.02). Onset age, duration of disease progression, neurological examinations, nerve conduction study, and electromyographic findings from individual muscles were similar between patient groups.Compared with HD patients without cord atrophy, HD patients with cord atrophy experience a more severe denervation change in C5 to C7 root-innervated muscles.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Sobue I, Saito N, Iida M, et al. Juvenile type of distal and segmental muscular atrophy of upper extremities. Ann Neurol 1978; 3:429–432. - PubMed
-
- Hirayama K. Juvenile muscular atrophy of distal upper extremity (Hirayama disease). Intern Med 2000; 39:283–290. - PubMed
-
- Huang YL, Chen CJ. Hirayama disease. Neuroimaging Clin N Am 2011; 21:939–950.ix–x. - PubMed
-
- Tashiro K, Kikuchi S, Itoyama Y, et al. Nationwide survey of juvenile muscular atrophy of distal upper extremity (Hirayama disease) in Japan. Amyotroph Lateral Scler 2006; 7:38–45. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
