

Stroke volume changes induced by a recruitment maneuver predict fluid responsiveness in patients with protective ventilation in the operating theater
- PMID: 27428237
- PMCID: PMC4956831
- DOI: 10.1097/MD.0000000000004259
Stroke volume changes induced by a recruitment maneuver predict fluid responsiveness in patients with protective ventilation in the operating theater
Abstract
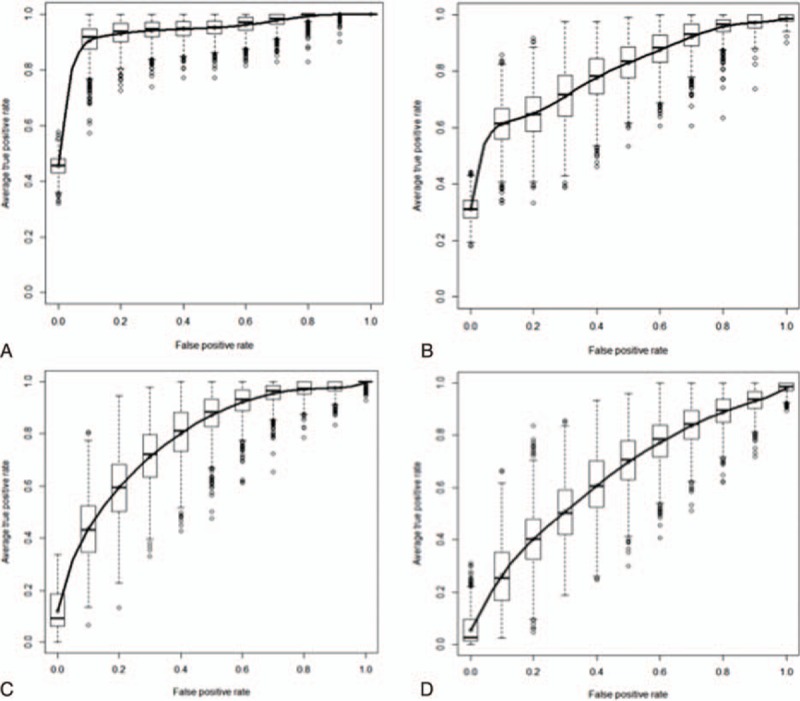
During abdominal surgery, the use of protective ventilation with a low tidal volume, positive expiratory pressure (PEEP) and recruitment maneuvers (RMs) may limit the applicability of dynamic preload indices. The objective of the present study was to establish whether or not the variation in stroke volume (SV) during an RM could predict fluid responsiveness.We prospectively included patients receiving protective ventilation (tidal volume: 6 mL kg, PEEP: 5-7 cmH2O; RMs). Hemodynamic variables, such as heart rate, arterial pressure, SV, cardiac output (CO), respiratory variation in SV (ΔrespSV) and pulse pressure (ΔrespPP), and the variation in SV (ΔrecSV) as well as pulse pressure (ΔrecPP) during an RM were measured at baseline, at the end of the RM, and after fluid expansion. Responders were defined as patients with an SV increase of at least 15% after infusion of 500 mL of crystalloid solution.Thirty-seven (62%) of the 60 included patients were responders. Responders and nonresponders differed significantly in terms of the median ΔrecSV (26% [19-37] vs 10% [4-12], respectively; P < 0.0001). A ΔrecSV value more than 16% predicted fluid responsiveness with an area under the receiver-operating characteristic curve (AU) of 0.95 (95% confidence interval [CI]: 0.91-0.99; P < 0.0001) and a narrow gray zone between 15% and 17%. The area under the curve values for ΔrecPP and ΔrespSV were, respectively, 0.81 (95%CI: 0.7-0.91; P = 0.0001) and 0.80 (95%CI: 0.70-0.94; P < 0.0001). ΔrespPP did not predict fluid responsiveness.During abdominal surgery with protective ventilation, a ΔrecSV value more than 16% accurately predicted fluid responsiveness and had a narrow gray zone (between 15% and 17%). ΔrecPP and ΔrespSV (but not ΔrespPP) were also predictive.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Hamilton MA, Cecconi M, Rhodes A. A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth Analg 2011; 112:1392–1402. - PubMed
-
- Perel A, Pizov R, Cotev S. Respiratory variations in the arterial pressure during mechanical ventilation reflect volume status and fluid responsiveness. Intensive Care Med 2014; 40:798–807. - PubMed
-
- Guerin L, Monnet X, Teboul JL. Monitoring volume and fluid responsiveness: from static to dynamic indicators. Best Pract Res Clin Anaesthesiol 2013; 27:177–185. - PubMed
-
- Futier E, Godet T, Millot A, et al. Mechanical ventilation in abdominal surgery. Ann Fr Anesth Reanim 2014; 33:472–475. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
