

Association of Serum Calprotectin (S100A8/A9) Level With Disease Relapse in Proteinase 3-Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
- PMID: 27428710
- PMCID: PMC5839649
- DOI: 10.1002/art.39814
Association of Serum Calprotectin (S100A8/A9) Level With Disease Relapse in Proteinase 3-Antineutrophil Cytoplasmic Antibody-Associated Vasculitis
Abstract
Objective: S100A8/A9 (calprotectin) has shown promise as a biomarker for predicting relapse in antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). This study was undertaken to investigate serum S100A8/A9 level as a biomarker for predicting future relapse in a large cohort of patients with severe AAV.
Methods: Serum levels of S100A8/A9 were measured at baseline and months 1, 2, and 6 following treatment initiation in 144 patients in the Rituximab in ANCA-Associated Vasculitis trial (cyclophosphamide/azathioprine versus rituximab [RTX] for induction of remission) in whom complete remission was attained.
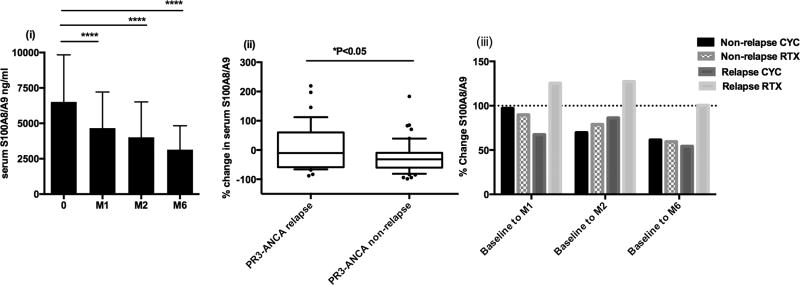
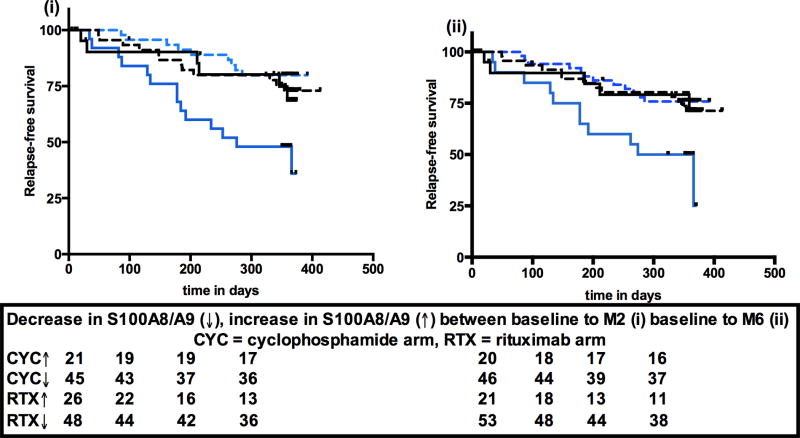
Results: Patients were divided into 4 groups: proteinase 3 (PR3)-ANCA with relapse (n = 37), PR3-ANCA without relapse (n = 56), myeloperoxidase (MPO)-ANCA with relapse (n = 6), and MPO-ANCA without relapse (n = 45). Serum S100A8/A9 level decreased in all groups during the first 6 months of treatment. The percentage reduction from baseline to month 2 was significantly different between patients who experienced a relapse and those who did not in the PR3-ANCA group (P = 0.046). A significantly higher risk of relapse was associated with an increase in S100A8/A9 level between baseline and month 2 (P = 0.0043) and baseline and month 6 (P = 0.0029). Subgroup analysis demonstrated that patients treated with RTX who had increased levels of S100A8/A9 were at greatest risk of future relapse (P = 0.028).
Conclusion: An increase in serum S100A8/A9 level by month 2 or 6 compared to baseline identifies a subgroup of PR3-ANCA patients treated with RTX who are at higher risk of relapse by 18 months. Since RTX is increasingly used for remission induction in PR3-ANCA-positive patients experiencing a relapse, S100A8/A9 level may assist in identifying those patients requiring more intensive or prolonged treatment.
© 2016, American College of Rheumatology.
Figures

References
-
- Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis and rheumatism. 1994;37(2):187–92. - PubMed
-
- Finkielman JD, Lee AS, Hummel AM, Viss MA, Jacob GL, Homburger HA, et al. ANCA are detectable in nearly all patients with active severe Wegener's granulomatosis. The American journal of medicine. 2007;120(7):643 e9–14. - PubMed
-
- Hagen EC, Daha MR, Hermans J, Andrassy K, Csernok E, Gaskin G, et al. Diagnostic value of standardized assays for anti-neutrophil cytoplasmic antibodies in idiopathic systemic vasculitis. EC/BCR Project for ANCA Assay Standardization. Kidney international. 1998;53(3):743–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
