

Indications and Efficacy of Gamma Knife Stereotactic Radiosurgery for Recurrent Glioblastoma: 2 Decades of Institutional Experience
- PMID: 27428784
- PMCID: PMC5235998
- DOI: 10.1227/NEU.0000000000001344
Indications and Efficacy of Gamma Knife Stereotactic Radiosurgery for Recurrent Glioblastoma: 2 Decades of Institutional Experience
Abstract
Background: The role of stereotactic radiosurgery (SRS) for recurrent glioblastoma and the radionecrosis risk in this setting remain unclear.
Objective: To perform a large retrospective study to help inform proper indications, efficacy, and anticipated complications of SRS for recurrent glioblastoma.
Methods: We retrospectively analyzed patients who underwent Gamma Knife SRS between 1991 and 2013. We used the partitioning deletion/substitution/addition algorithm to identify potential predictor covariate cut points and Kaplan-Meier and proportional hazards modeling to identify factors associated with post-SRS and postdiagnosis survival.
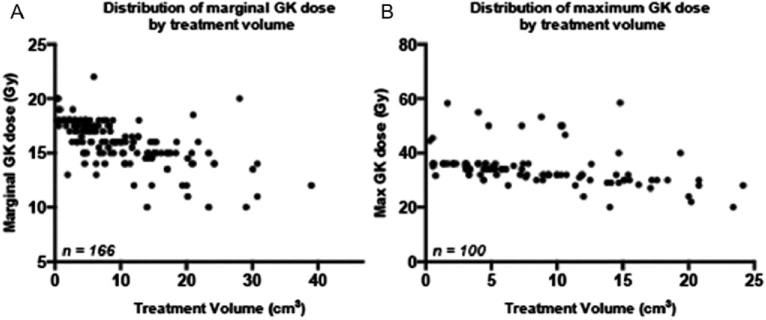
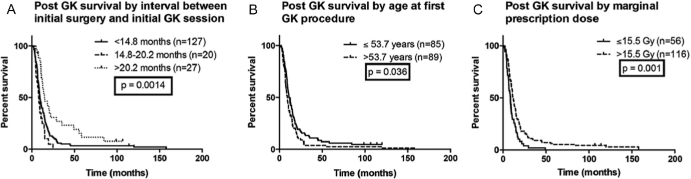
Results: One hundred seventy-four glioblastoma patients (median age, 54.1 years) underwent SRS a median of 8.7 months after initial diagnosis. Seventy-five percent had 1 treatment target (range, 1-6), and median target volume and prescriptions were 7.0 cm 3 (range, 0.3-39.0 cm 3 ) and 16.0 Gy (range, 10-22 Gy), respectively. Median overall survival was 10.6 months after SRS and 19.1 months after diagnosis. Kaplan-Meier and multivariable modeling revealed that younger age at SRS, higher prescription dose, and longer interval between original surgery and SRS are significantly associated with improved post-SRS survival. Forty-six patients (26%) underwent salvage craniotomy after SRS, with 63% showing radionecrosis or mixed tumor/necrosis vs 35% showing purely recurrent tumor. The necrosis/mixed group had lower mean isodose prescription compared with the tumor group (16.2 vs 17.8 Gy; P = .003) and larger mean treatment volume (10.0 vs 5.4 cm 3 ; P = .009).
Conclusion: Gamma Knife may benefit a subset of focally recurrent patients, particularly those who are younger with smaller recurrences. Higher prescriptions are associated with improved post-SRS survival and do not seem to have greater risk of symptomatic treatment effect.
Keywords: Gamma knife; Glioblastoma; Radionecrosis; Recurrent; SRS; Stereotactic radiosurgery.
Copyright © 2016 by the Congress of Neurological Surgeons
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987-996. - PubMed
-
- Niyazi M, Siefert A, Schwarz SB et al. Therapeutic options for recurrent malignant glioma. Radiother Oncol. 2011;98(1):1-14. - PubMed
-
- Young B, Oldfield EH, Markesbery WR et al. Reoperation for glioblastoma. J Neurosurg. 1981;55(6):917-921. - PubMed
-
- Ammirati M, Galicich JH, Arbit E, Liao Y. Reoperation in the treatment of recurrent intracranial malignant gliomas. Neurosurgery. 1987;21(5):607-614. - PubMed
-
- Harsh GR, Levin VA, Gutin PH, Seager M, Silver P, Wilson CB. Reoperation for recurrent glioblastoma and anaplastic astrocytoma. Neurosurgery. 1987;21(5):615-621. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
