

Changes in Functional Mobility and Musculoskeletal Pain After Bariatric Surgery in Teens With Severe Obesity: Teen-Longitudinal Assessment of Bariatric Surgery (LABS) Study
- PMID: 27429076
- PMCID: PMC5904853
- DOI: 10.1001/jamapediatrics.2016.1196
Changes in Functional Mobility and Musculoskeletal Pain After Bariatric Surgery in Teens With Severe Obesity: Teen-Longitudinal Assessment of Bariatric Surgery (LABS) Study
Abstract
Importance: Severe obesity is associated with mobility limitations and higher incidence of multijoint musculoskeletal pain. It is unknown whether substantial weight loss improves these important outcomes in adolescents with severe obesity.
Objective: To examine the association of bariatric surgery with functional mobility and musculoskeletal pain in adolescents with severe obesity up to 2 years after surgery.
Design, setting, and participants: The Teen-Longitudinal Assessment of Bariatric Surgery Study is a prospective, multicenter, observational study, which enrolled 242 adolescents (≤19 years of age) who were undergoing bariatric surgery from March 2007 through February 2012 at 5 US adolescent bariatric surgery centers. This analysis was conducted in November 2015.
Interventions: Roux-en-Y gastric bypass (n = 161), sleeve gastrectomy (n = 67), or laparoscopic adjustable gastric band (n = 14).
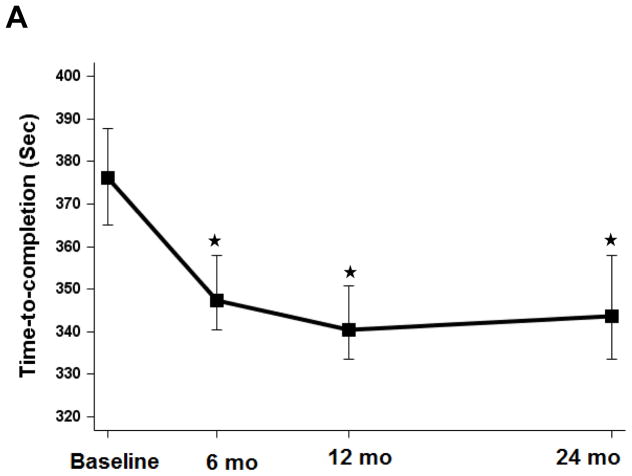
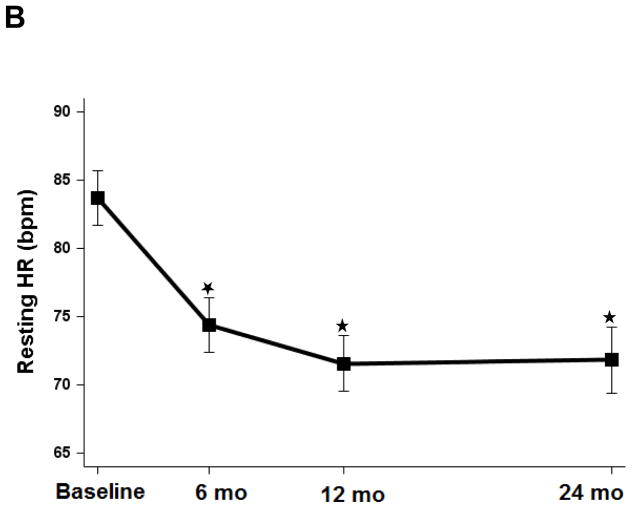
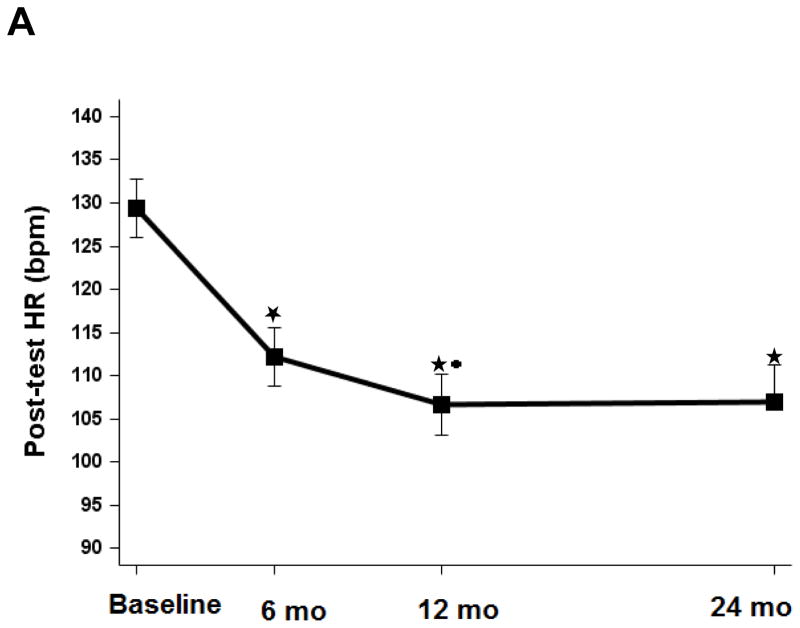
Main outcomes and measures: Participants completed a 400-m walk test prior to bariatric surgery (n = 206) and at 6 months (n = 195), 12 months (n = 176), and 24 months (n = 149) after surgery. Time to completion, resting heart rate (HR), immediate posttest HR, and HR difference (resting HR minus posttest HR) were measured and musculoskeletal pain concerns, during and after the test, were documented. Data were adjusted for age, sex, race/ethnicity, baseline body mass index (calculated as weight in kilograms divided by height in meters squared), and surgical center (posttest HR and HR difference were further adjusted for changes in time to completion).
Results: Of the 206 adolescents with severe obesity included in the study, 156 were female (75.7%), the mean (SD) age was 17.1 (1.6) years, and the mean (SD) body mass index was 51.7 (8.5). Compared with baseline, significant improvements were observed at 6 months for the walk test time to completion (mean, 376 seconds; 95% CI, 365-388 to 347 seconds; 95% CI, 340-358; P < .01), resting HR (mean, 84 beats per minute [bpm]; 95% CI, 82-86 to 74 bpm; 95% CI, 72-76), posttest HR (mean, 128 bpm; 95% CI, 125-131 to 113 bpm; 95% CI, 110-116), and HR difference (mean, 40 bpm; 95% CI, 36-42 to 34 bpm; 95% CI, 31-37). These changes in time to completion, resting HR, and HR difference persisted at 12 months and 24 months. Posttest HR further improved from 6 months to 12 months (mean, 113 bpm; 95% CI, 110-116 to 108 bpm; 95% CI, 105-111). There were statistically significant reductions in musculoskeletal pain concerns at all points.
Conclusions and relevance: These data provide evidence that bariatric surgery in adolescents with severe obesity is associated with significant improvement in functional mobility and in the reduction of walking-related musculoskeletal pain up to 2 years after surgery.
Figures
 indicating p=0.10 from 6mo.
indicating p=0.10 from 6mo.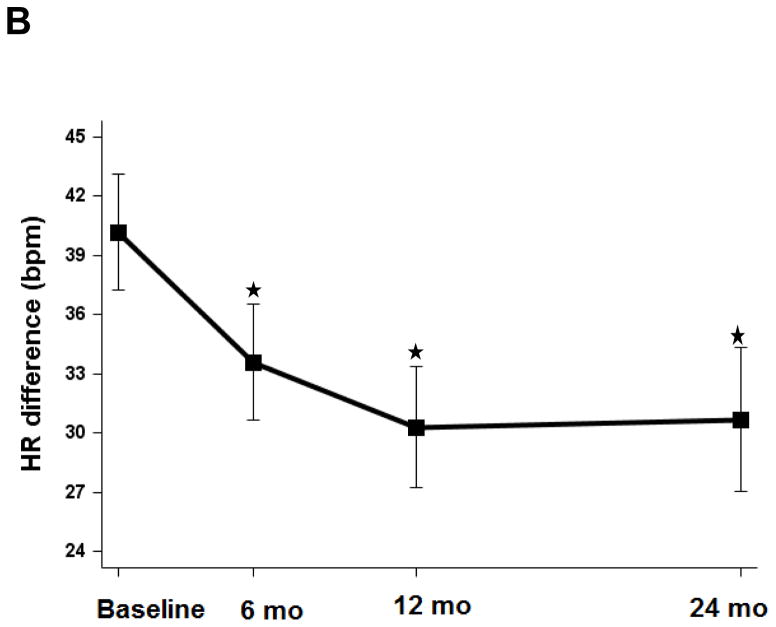 indicating p=0.10 from 6mo.
indicating p=0.10 from 6mo.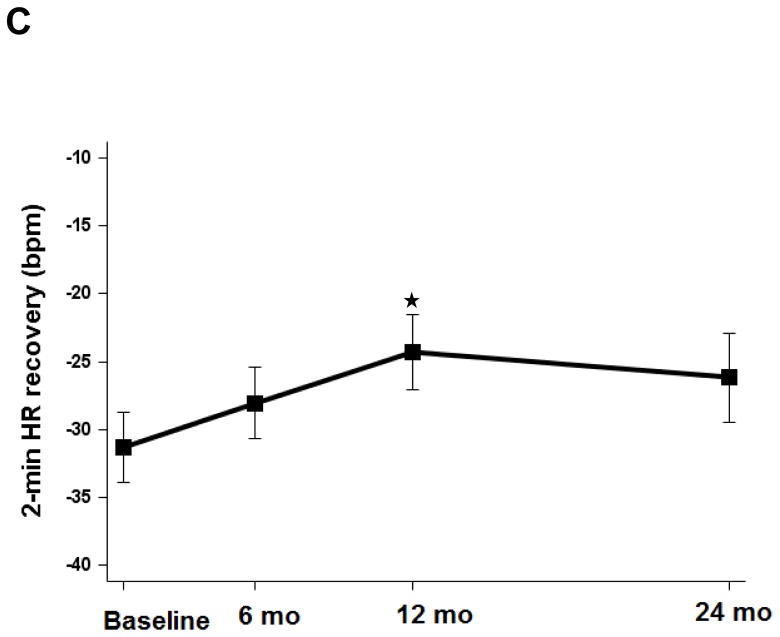 indicating p=0.10 from 6mo.
indicating p=0.10 from 6mo.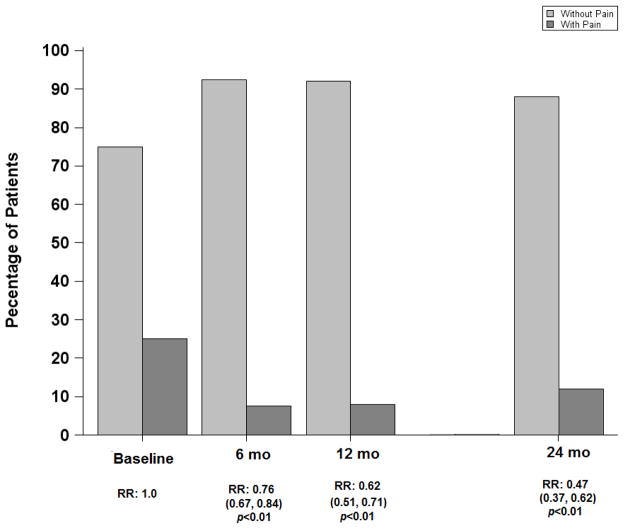
Similar articles
-
Functional mobility and pain are improved for 6 years after adolescent bariatric surgery.Obesity (Silver Spring). 2025 Jun;33(6):1126-1135. doi: 10.1002/oby.24285. Epub 2025 Apr 21. Obesity (Silver Spring). 2025. PMID: 40259728 Free PMC article.
-
Musculoskeletal Pain, Self-reported Physical Function, and Quality of Life in the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) Cohort.JAMA Pediatr. 2015 Jun;169(6):552-9. doi: 10.1001/jamapediatrics.2015.0378. JAMA Pediatr. 2015. PMID: 25915190 Free PMC article.
-
Perioperative outcomes of adolescents undergoing bariatric surgery: the Teen-Longitudinal Assessment of Bariatric Surgery (Teen-LABS) study.JAMA Pediatr. 2014 Jan;168(1):47-53. doi: 10.1001/jamapediatrics.2013.4296. JAMA Pediatr. 2014. PMID: 24189578 Free PMC article. Clinical Trial.
-
Bariatric surgery for the management of obesity: state of the field.Plast Reconstr Surg. 2012 Oct;130(4):948-954. doi: 10.1097/PRS.0b013e318262f566. Plast Reconstr Surg. 2012. PMID: 23018704 Review.
-
Obesity in Adolescents: A Review.JAMA. 2024 Sep 3;332(9):738-748. doi: 10.1001/jama.2024.11809. JAMA. 2024. PMID: 39102244 Review.
Cited by
-
Loss of Control Eating and Health Indicators Over 6 Years in Adolescents Undergoing Metabolic and Bariatric Surgery.Obesity (Silver Spring). 2021 Apr;29(4):740-747. doi: 10.1002/oby.23126. Obesity (Silver Spring). 2021. PMID: 33759383 Free PMC article.
-
Short- and long-term safety and efficacy of bariatric surgery for severely obese adolescents: a narrative review.Pediatr Res. 2020 Jan;87(2):202-209. doi: 10.1038/s41390-019-0532-3. Epub 2019 Aug 11. Pediatr Res. 2020. PMID: 31401646 Review.
-
Obesity in children and adolescents: epidemiology, causes, assessment, and management.Lancet Diabetes Endocrinol. 2022 May;10(5):351-365. doi: 10.1016/S2213-8587(22)00047-X. Epub 2022 Mar 3. Lancet Diabetes Endocrinol. 2022. PMID: 35248172 Free PMC article. Review.
-
Changes in Myokines in Youths With Severe Obesity Following Roux-en-Y Gastric Bypass Surgery.JAMA Surg. 2019 Jul 1;154(7):668-669. doi: 10.1001/jamasurg.2019.0424. JAMA Surg. 2019. PMID: 30969334 Free PMC article.
-
Functional mobility and pain are improved for 6 years after adolescent bariatric surgery.Obesity (Silver Spring). 2025 Jun;33(6):1126-1135. doi: 10.1002/oby.24285. Epub 2025 Apr 21. Obesity (Silver Spring). 2025. PMID: 40259728 Free PMC article.
References
-
- Gidding SS, Nehgme R, Heise C, Muscar C, Linton A, Hassink S. Severe obesity associated with cardiovascular deconditioning, high prevalence of cardiovascular risk factors, diabetes mellitus/hyperinsulinemia, and respiratory compromise. The Journal of Pediatrics. 2004;144(6):766–769. - PubMed
-
- Stovitz SD, Pardee PE, Vazquez G, Duval S, Schwimmer JB. Musculoskeletal pain in obese children and adolescents. Acta Pædiatrica. 2008;97(4):489–493. - PubMed
-
- Wearing SC, Hennig EM, Byrne NM, Steele JR, Hills AP. The impact of childhood obesity on musculoskeletal form. Obesity Reviews. 2006;7(2):209–218. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
