

Distinct Subtypes of Behavioral Variant Frontotemporal Dementia Based on Patterns of Network Degeneration
- PMID: 27429218
- PMCID: PMC5024785
- DOI: 10.1001/jamaneurol.2016.2016
Distinct Subtypes of Behavioral Variant Frontotemporal Dementia Based on Patterns of Network Degeneration
Abstract
Importance: Clearer delineation of the phenotypic heterogeneity within behavioral variant frontotemporal dementia (bvFTD) will help uncover underlying biological mechanisms and improve clinicians' ability to predict disease course and to design targeted management strategies.
Objective: To identify subtypes of bvFTD syndrome based on distinctive patterns of atrophy defined by selective vulnerability of specific functional networks targeted in bvFTD using statistical classification approaches.
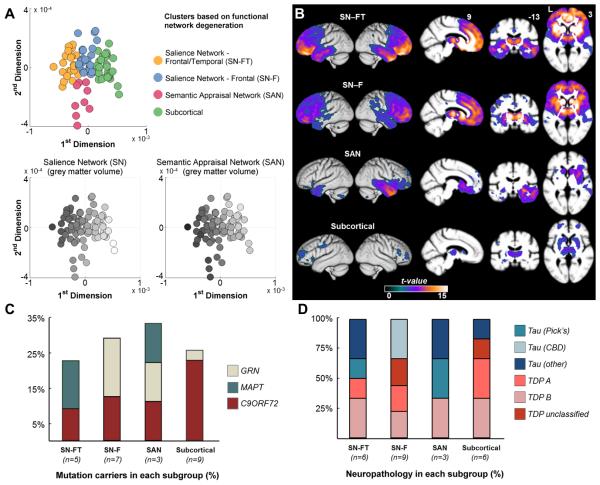
Design, setting and participants: In this retrospective observational study, 90 patients meeting the Frontotemporal Dementia Consortium consensus criteria for bvFTD underwent evaluation at the Memory and Aging Center of the Department of Neurology at University of California, San Francisco. Patients underwent a multidisciplinary clinical evaluation, including clinical demographics, genetic testing, symptom evaluation, neurologic examination, neuropsychological bedside testing, and socioemotional assessments. All patients underwent structural magnetic resonance imaging at their earliest evaluation at the memory clinic. From each patient's structural imaging scans, the mean volumes of 18 regions of interest (ROI) constituting the functional networks specifically vulnerable in bvFTD, including the salience network (SN), with key nodes in the frontoinsula and pregenual anterior cingulate, and the semantic appraisal network (SAN), anchored in the anterior temporal lobe and subgenual cingulate, were estimated. Principal component and cluster analyses of ROI volumes were used to identify patient clusters with anatomically distinct atrophy patterns. Data were collected from from June 19, 2002, to January 13, 2015.
Main outcomes and measures: Evaluation of brain morphology and other clinical features, including presenting symptoms, neurologic examination signs, neuropsychological performance, rate of dementia progression, and socioemotional function, in each patient cluster.
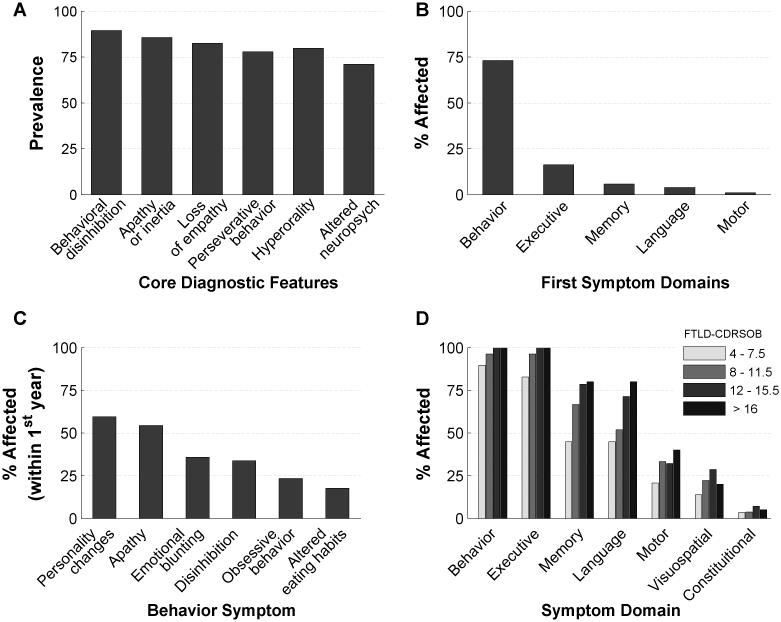
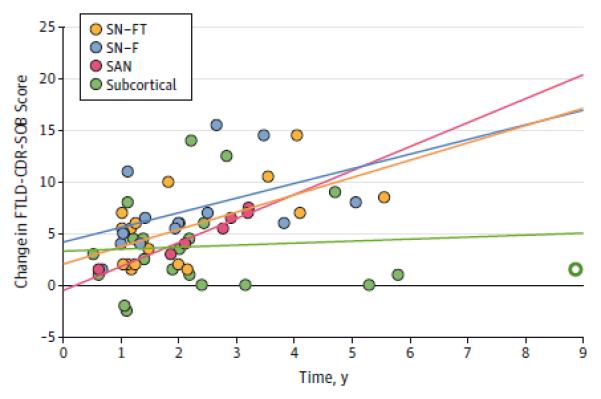
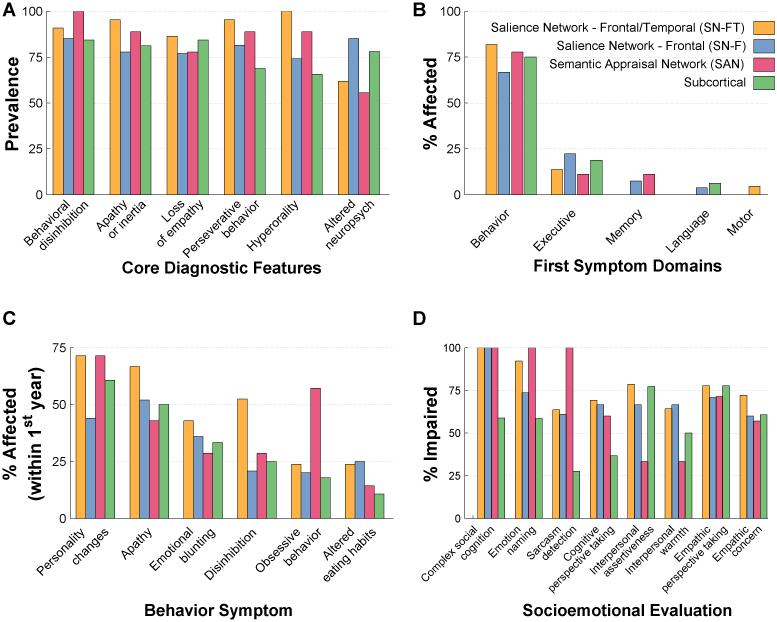
Results: Ninety patients (54 men [60%]; 36 women [40%]; mean [SD] age at evaluation, 55.1 [9.7] years) were included in the analysis. Four subgroups of patients with bvFTD with distinct anatomic patterns of network degeneration were identified, including 2 salience network-predominant subgroups (frontal/temporal [SN-FT] and frontal [SN-F]), a semantic appraisal network-predominant group (SAN), and a subcortical-predominant group. Subgroups demonstrated distinct patterns of cognitive, socioemotional, and motor symptoms, as well as genetic compositions and estimated rates of disease progression.
Conclusions and relevance: Divergent patterns of vulnerability in specific functional network components make an important contribution to the clinical heterogeneity of bvFTD. The data-driven anatomic classification identifies biologically meaningful anatomic phenotypes and provides a replicable approach to disambiguate the bvFTD syndrome.
Figures
Comment in
-
Behavioral Variant Frontotemporal Dementia: One Syndrome, Several Circuits, Many Mechanisms.JAMA Neurol. 2016 Sep 1;73(9):1051-2. doi: 10.1001/jamaneurol.2016.1793. JAMA Neurol. 2016. PMID: 27428243 No abstract available.
References
-
- Neary D, Snowden JS, Gustafson L, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51(6):1546–1554. - PubMed
-
- Snowden JS, Neary D, Mann DM. Frontotemporal dementia. Br J Psychiatry. 2002;180:140–143. - PubMed
-
- Hodges JR. Frontotemporal dementia (Pick's disease): clinical features and assessment. Neurology. 2001;56(11 Suppl 4):S6–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 AG040127/AG/NIA NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
- K23 AG039414/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- K23 AG021606/AG/NIA NIH HHS/United States
- K23 AG045289/AG/NIA NIH HHS/United States
- K23 AG042492/AG/NIA NIH HHS/United States
- R01 NS050915/NS/NINDS NIH HHS/United States
- U54 NS092089/NS/NINDS NIH HHS/United States
- R01 AG032306/AG/NIA NIH HHS/United States
- K23 AG038357/AG/NIA NIH HHS/United States
- RF1 AG029577/AG/NIA NIH HHS/United States
- R01 AG029577/AG/NIA NIH HHS/United States
- L30 RR022879/RR/NCRR NIH HHS/United States
- K24 DC015544/DC/NIDCD NIH HHS/United States
- U01 AG052943/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- K23 AG037566/AG/NIA NIH HHS/United States
- L30 AG038306/AG/NIA NIH HHS/United States
- K23 AG048291/AG/NIA NIH HHS/United States
