

Therapeutic Progress in Treating Vertebral Dissecting Aneurysms Involving the Posterior Inferior Cerebellar Artery
- PMID: 27429591
- PMCID: PMC4946125
- DOI: 10.7150/ijms.15233
Therapeutic Progress in Treating Vertebral Dissecting Aneurysms Involving the Posterior Inferior Cerebellar Artery
Abstract
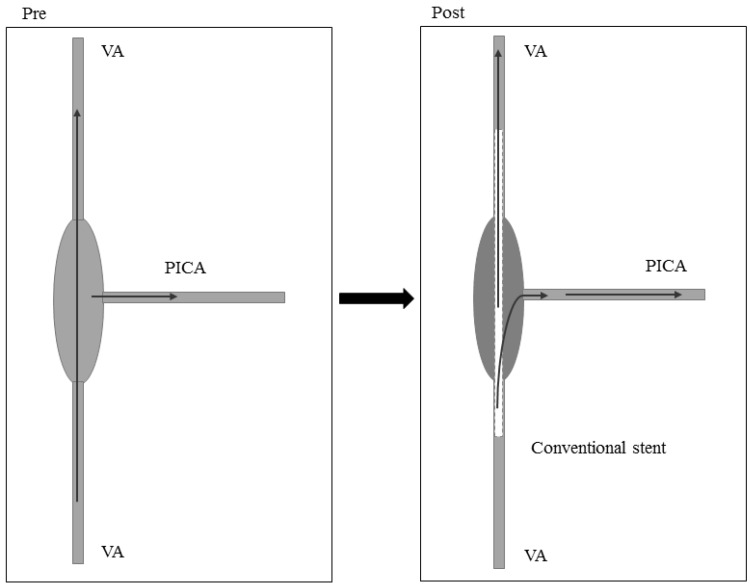
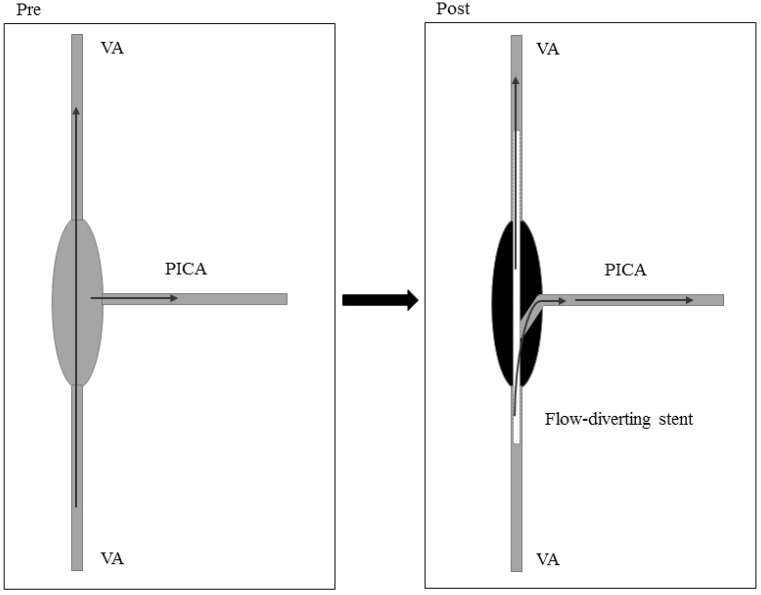
Among the variations of vertebral artery dissecting aneurysms (VDAs), VDAs involving the posterior inferior cerebellar artery (PICA), especially ruptured and high-risk unruptured aneurysms, are the most difficult to treat. Because the PICA is an important structure, serious symptoms may occur after its occlusion. Retained PICAs are prone to re-bleeding because VDAs are difficult to completely occlude. There is therefore confusion regarding the appropriate treatment for VDAs involving the PICA. Here, we used the PubMed database to review recent research concerning VDAs that involve the PICA, and we found that treatments for VDAs involving the PICA include (i) endovascular treatment involving the reconstruction of blood vessels and blood flow, (ii) occluding the aneurysm using an internal coil trapping or an assisted bypass, (iii) inducing reversed blood flow by occluding the proximal VDA or forming an assisted bypass, or (iv) the reconstruction of blood flow via a craniotomy. Although the above methods effectively treat VDAs involving the PICA, each method is associated with both a high degree of risk and specific advantages and disadvantages. The core problem when treating VDAs involving the PICA is to retain the PICA while occluding the aneurysm. Therefore, the method is generally selected on a case-by-case basis according to the characteristics of the aneurysm. In this study, we summarize the various current methods that are used to treat VDAs involving the PICA and provide schematic diagrams as our conclusion. Because there is no special field of research concerning VDAs involving the PICA, these cases are hidden within many multiple-cases studies. Therefore, this study does not review all relevant documents and may have some limitations. Thus, we have focused on the mainstream treatments for VDAs that involve the PICA.
Keywords: Vertebral artery dissecting aneurysms; posterior inferior cerebellar artery; therapeutic progress..
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures













References
-
- Hernandez-Duran S, Ogilvy CS. Clinical outcomes of patients with vertebral artery dissection treated endovascularly: a meta-analysis. Neurosurg Rev. 2014;37:569–77. - PubMed
-
- Iihara K, Sakai N, Murao K, Sakai H, Higashi T, Kogure S. et al. Dissecting aneurysms of the vertebral artery: a management strategy. J Neurosurg. 2002;97:259–67. - PubMed
-
- Fine AD, Cardoso A, Rhoton AL Jr. Microsurgical anatomy of the extracranial-extradural origin of the posterior inferior cerebellar artery. J Neurosurg. 1999;91:645–52. - PubMed
-
- Matsukawa H, Shinoda M, Fujii M, Takahashi O, Uemura A, Niimi Y. Basilar extension and posterior inferior cerebellar artery involvement as risk factors for progression of the unruptured spontaneous intradural vertebral artery dissection. J Neurol Neurosurg Psychiatry. 2014;85:1049–54. - PubMed
-
- Sano H, Kato Y, Okuma I, Yamaguchi S, Ninomiya T, Arunkumar R. et al. Classification and treatment of vertebral dissecting aneurysm. Surg Neurol. 1997;48:598–605. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
