

Recognizing IgG4-related tubulointerstitial nephritis
- PMID: 27429760
- PMCID: PMC4947514
- DOI: 10.1186/s40697-016-0126-5
Recognizing IgG4-related tubulointerstitial nephritis
Abstract
Purpose of the review: Immunoglobulin G4-related disease (IgG4-RD) is a systemic fibroinflammatory disorder affecting nearly all organs, including the kidney. Tubulointerstitial nephritis (IgG4-TIN) is the most common form of IgG4-related kidney disease (IgG4-RKD) and is the focus of this concise review.
Objective: The study aims to describe when IgG4-TIN should be suspected and to summarize the diagnosis, treatment, and natural history of the disease.
Sources of information: Ovid MEDLINE, Google Scholar, and PubMed were searched for full-text English language articles up to January 2016. References included in the manuscript were chosen at the authors' discretion based on their relevance to the subject of the review.
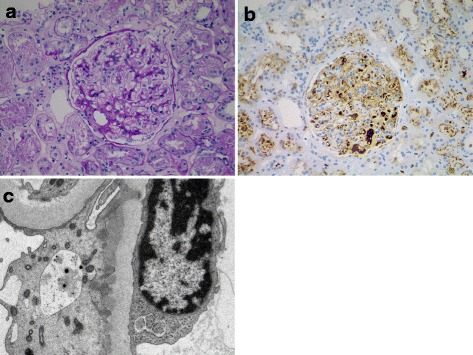
Findings: IgG4-TIN should be considered in patients presenting with abnormal urinalysis, abnormal kidney function, renal lesions on imaging, and elevated IgG, IgE, or hypocomplementemia. Diagnosis of IgG4-TIN requires a combination of histologic features (plasma cell-enriched TIN with >10 IgG4+ plasma cells/hpf, +/- TBM immune complex deposits in many cases) and at least one of the following:Characteristic radiologic findings (small peripheral low-attenuation cortical nodules, round or wedge-shaped lesions, or diffuse patchy involvement)Elevated serum IgG4 levelCharacteristic findings of IgG4-RD in other organs Other conditions such as lupus, vasculitis, diabetic nephropathy, and lymphoma must be excluded, as these can also present with IgG4+ plasma cells in the renal parenchyma. IgG4-TIN is generally responsive to steroids and B cell depletion with rituximab, but relapses are common and patients require close long-term follow-up.
Limitations: Available data on IgG4-TIN are from retrospective observational studies.
Implications: IgG4-TIN is a distinct and emerging subtype of interstitial nephritis. Nephrologists must be aware of this entity and how to definitively diagnose and treat it. Prospective studies and ideally multi-center clinical trials are needed to study the epidemiology, treatment, and natural history of this disease.
Motif de la revue: Les maladies associées aux immuglobulines G4 (IgG4) sont caractérisées par un désordre systémique d’ordre fibro-inflammatoire qui affecte pratiquement tous les organes, incluant les reins. La néphropathie tubulo-interstitielle (tubulointerstitial nephritis: IgG4-TIN), qui fait l’objet de la présente revue, est la maladie rénale associée aux IgG4 la plus fréquemment observée.
Objectif de la revue: On a voulu faire le portrait de la néphropathie tubulo-interstitielle (IgG4-TIN) telle que nous la comprenons actuellement: les signes cliniques indiquant sa possible présence, les indices permettant son diagnostic, ainsi que le traitement et l’évolution naturelle de cette maladie.
Sources: Tous les articles publiés en anglais sur ce sujet jusqu’en janvier 2016 ont été répertoriés sur Ovid MEDLINE, Google Scholar et PubMed. Les références choisies pour la présente revue ont été sélectionnées à la discrétion des auteurs, sur la base de leur pertinence au sujet.
Constat: Une IgG4-TIN devrait être suspectée chez les patients présentant des anormalités lors d’une analyse d’urine, des troubles de la fonction rénale, des lésions aux reins observables par imagerie, des taux élevés d’IgG, d’IgE ou une hypocomplémentémie. Le diagnostic d’une IgG4-TIN demande la combinaison de paramètres histologiques (infiltrat tubulo-interstitiel riche en plasmocytes, avec >10 plasmocytes IgG4+ par HPF, avec ou sans dépôts de complexes immuns dans la membrane basale tubulaire) ainsi qu’au moins une des manifestations suivantes:l’observation radiologique d'indices caractéristiques de la maladie (nodules corticaux périphériques de faible atténuation, cunéiformes ou d’atteinte inégale et diffuse)des taux élevés d’IgG4 sériquesla présence d’une maladie associée aux IgG4 dans d’autres organes Les maladies telles que le lupus, la vascularite, la néphropathie diabétique ou les lymphomes sont exclues puisque celles-ci sont également caractérisées par une présence élevée de plasmocytes sécréteurs d’IgG4 au niveau du parenchyme rénal. De façon générale, l’IgG4-TIN répond bien aux stéroïdes et à une déplétion des lymphocytes B avec le rituximab, mais les récidives sont fréquentes et les patients requièrent un suivi étroit et à long terme.
Limites de l’étude: Les données colligées sur la néphropathie tubulo-interstitielle pour cette revue proviennent d’études observationnelles rétrospectives.
Conclusion: L’IgG4-TIN est un sous-type émergent et distinct de néphropathie interstitielle que les néphrologues doivent pouvoir identifier, diagnostiquer et traiter. Des études prospectives, idéalement des essais cliniques impliquant plusieurs centres de soins, sont nécessaires pour étudier l’épidémiologie et déterminer le traitement et l’évolution naturelle de cette maladie.
Keywords: Autoimmune tubulointerstitial nephritis; Epidemiology; IgG4-related disease; IgG4-related kidney disease; IgG4-related tubulointerstitial nephritis; Tubulointerstitial nephritis.
Figures

References
-
- Chen L. Does this patient have IgG4 related disease? Journal of Canadian Rheumatology Association. 2015;25(1):26–8.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
