

Serrated polyposis associated with a family history of colorectal cancer and/or polyps: The preferential location of polyps in the colon and rectum defines two molecular entities
- PMID: 27430658
- PMCID: PMC4990292
- DOI: 10.3892/ijmm.2016.2666
Serrated polyposis associated with a family history of colorectal cancer and/or polyps: The preferential location of polyps in the colon and rectum defines two molecular entities
Abstract
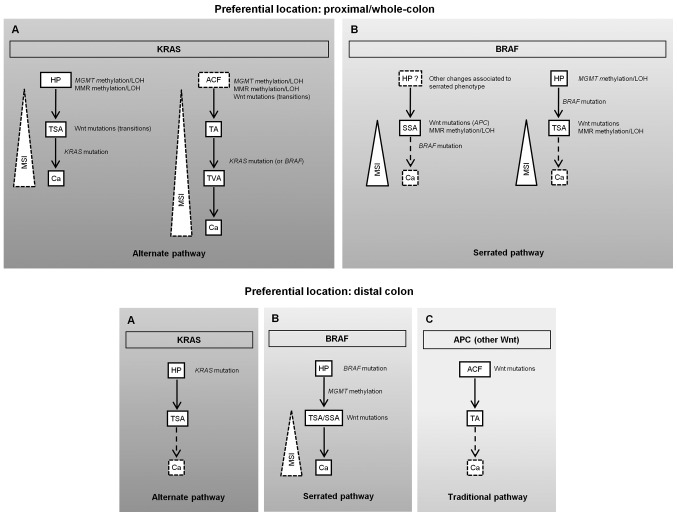
Serrated polyposis (SPP) is characterized by the development of multiple serrated polyps and an increased predisposition to colorectal cancer (CRC). In the present study, we aimed to characterize, at a clinical and molecular level, a cohort of SPP patients with or without a family history of SPP and/or polyps/CRC (SPP-FHP/CRC). Sixty-two lesions from 12 patients with SPP-FHP/CRC and 6 patients with sporadic SPP were included. The patients with SPP-FHP/CRC presented with an older mean age at diagnosis (p=0.027) and a more heterogeneous histological pattern of lesions (p=0.032) than the patients with sporadic SPP. We identified two molecular forms of SPP-FHP/CRC, according to the preferential location of the lesions: proximal/whole-colon or distal colon. Mismatch repair (MMR) gene methylation [mutS homolog 6 (MSH6)/mutS homolog 3 (MSH3)] or loss of heterozygosity (LOH) of D2S123 (flanking MSH6) were detected exclusively in the former (p=3.0x10-7), in most early lesions. Proximal/whole‑colon SPP-FHP/CRC presented a higher frequency of O-6-methylguanine-DNA methyltransferase (MGMT) methylation/LOH, microsatellite instability (MSI) and Wnt mutations (19/29 vs. 7/17; 16/23 vs. 1/14, p=2.2x10-4; 15/26 vs. 2/15, p=0.006; 14/26 vs. 4/20, p=0.02) but a lower frequency of B-raf proto-oncogene, serine/threonine kinase (BRAF) mutations (7/30 vs. 12/20, p=0.0089) than the distal form. CRC was more frequent in cases of Kirsten rat sarcoma viral oncogene homolog (KRAS)-associated proximal/whole-colon SPP-FHP/CRC than in the remaining cases (4/4 vs. 1/8, p=0.01). Thus, SPP-FHP/CRC appears to be a specific entity, presenting two forms, proximal/whole-colon and distal, which differ in the underlying tumor initiation pathways. Early MGMT and MMR gene deficiency in the former may underlie an inherited susceptibility to genotoxic stress.
Figures
Similar articles
-
Molecular features of colorectal hyperplastic polyps and sessile serrated adenoma/polyps from Korea.Am J Surg Pathol. 2011 Sep;35(9):1274-86. doi: 10.1097/PAS.0b013e318224cd2e. Am J Surg Pathol. 2011. PMID: 21836485
-
[Immunophenotypes and gene mutations in colorectal precancerous lesions and adenocarcinoma].Zhonghua Bing Li Xue Za Zhi. 2013 Oct;42(10):655-9. Zhonghua Bing Li Xue Za Zhi. 2013. PMID: 24433726 Chinese.
-
Colorectal carcinomas with KRAS mutation are associated with distinctive morphological and molecular features.Mod Pathol. 2013 Jun;26(6):825-34. doi: 10.1038/modpathol.2012.240. Epub 2013 Jan 25. Mod Pathol. 2013. PMID: 23348904
-
Colorectal serrated adenocarcinoma.Histopathology. 2007 Jan;50(1):131-50. doi: 10.1111/j.1365-2559.2006.02548.x. Histopathology. 2007. PMID: 17204027 Review.
-
[Colorectal serrated lesions: current insight on their role in colorectal carcinogenesis].Duodecim. 2010;126(17):2002-11. Duodecim. 2010. PMID: 21053517 Review. Finnish.
Cited by
-
Patient-Derived Explants of Colorectal Cancer: Histopathological and Molecular Analysis of Long-Term Cultures.Cancers (Basel). 2021 Sep 19;13(18):4695. doi: 10.3390/cancers13184695. Cancers (Basel). 2021. PMID: 34572922 Free PMC article.
-
Routine Immunohistochemical Analysis of Mismatch Repair Proteins in Colorectal Cancer-A Prospective Analysis.Cancers (Basel). 2022 Jul 31;14(15):3730. doi: 10.3390/cancers14153730. Cancers (Basel). 2022. PMID: 35954394 Free PMC article.
-
Germline Variants in DNA Interstrand-Cross Link Repair Genes May Contribute to Increased Susceptibility for Serrated Polyposis Syndrome.Int J Mol Sci. 2024 Nov 4;25(21):11848. doi: 10.3390/ijms252111848. Int J Mol Sci. 2024. PMID: 39519399 Free PMC article.
References
-
- Snover DC, Ahnen DJ, Burt RW, Odze RD. Serrated polyps of the colon and rectum and serrated polyposis. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO Classification of Tumours of the Digestive System. IARC; Lyon: 2010. pp. 160–165.
-
- Aust DE, Baretton GB, Members of the Working Group GI-Pathology of the German Society of Pathology Serrated polyps of the colon and rectum (hyperplastic polyps, sessile serrated adenomas, traditional serrated adenomas, and mixed polyps)-proposal for diagnostic criteria. Virchows Arch. 2010;457:291–297. doi: 10.1007/s00428-010-0945-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
