

Daptomycin Improves Outcomes Regardless of Vancomycin MIC in a Propensity-Matched Analysis of Methicillin-Resistant Staphylococcus aureus Bloodstream Infections
- PMID: 27431221
- PMCID: PMC5038271
- DOI: 10.1128/AAC.00227-16
Daptomycin Improves Outcomes Regardless of Vancomycin MIC in a Propensity-Matched Analysis of Methicillin-Resistant Staphylococcus aureus Bloodstream Infections
Abstract
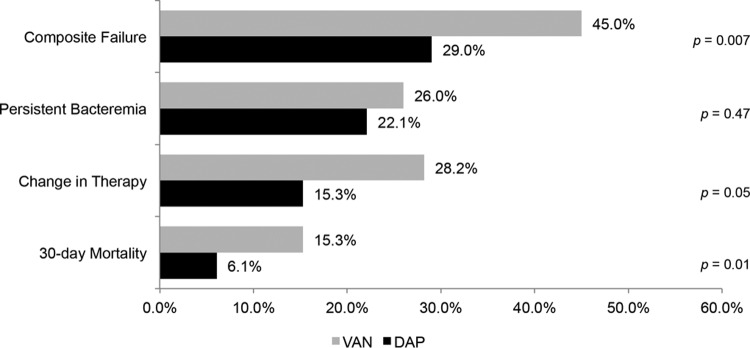
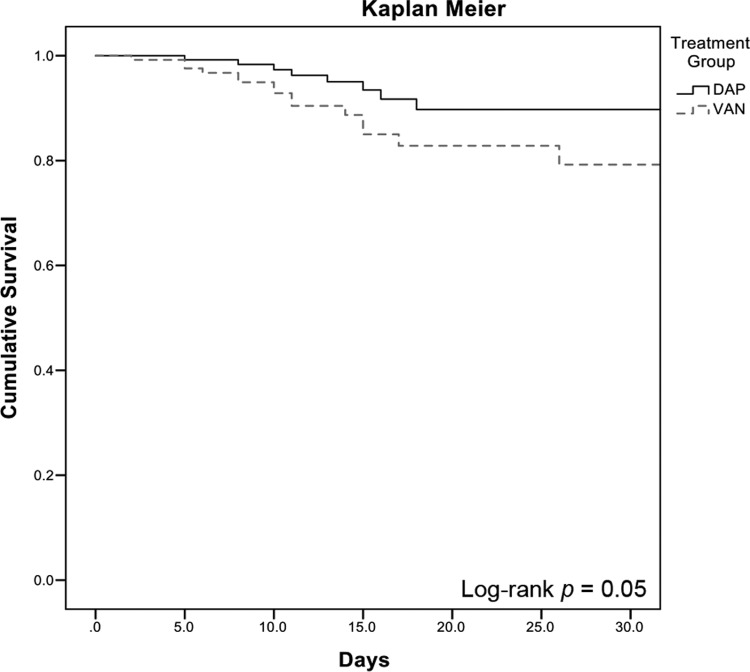
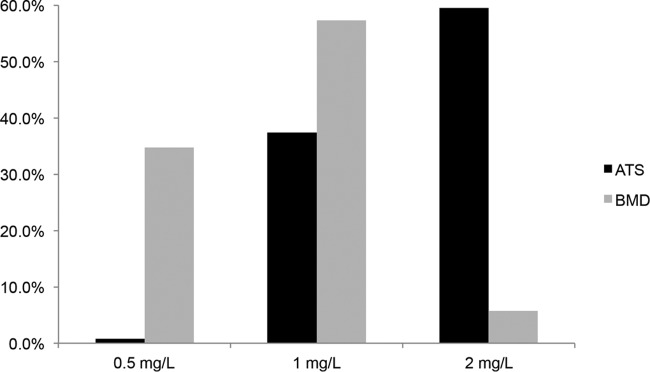
Vancomycin remains the mainstay treatment for methicillin-resistant Staphylococcus aureus (MRSA) bloodstream infections (BSIs) despite increased treatment failures. Daptomycin has been shown to improve clinical outcomes in patients with BSIs caused by MRSA isolates with vancomycin MICs of >1 mg/liter, but these studies relied on automated testing systems. We evaluated the outcomes of BSIs caused by MRSA isolates for which vancomycin MICs were determined by standard broth microdilution (BMD). A retrospective, matched cohort of patients with MRSA BSIs treated with vancomycin or daptomycin from January 2010 to March 2015 was completed. Patients were matched using propensity-adjusted logistic regression, which included age, Pitt bacteremia score, primary BSI source, and hospital of care. The primary endpoint was clinical failure, which was a composite endpoint of the following metrics: 30-day mortality, bacteremia with a duration of ≥7 days, or a change in anti-MRSA therapy due to persistent or worsening signs or symptoms. Secondary endpoints included MRSA-attributable mortality and the number of days of MRSA bacteremia. Independent predictors of failure were determined through conditional backwards-stepwise logistic regression with vancomycin BMD MIC forced into the model. A total of 262 patients were matched. Clinical failure was significantly higher in the vancomycin cohort than in the daptomycin cohort (45.0% versus 29.0%; P = 0.007). All-cause 30-day mortality was significantly higher in the vancomycin cohort (15.3% versus 6.1%; P = 0.024). These outcomes remained significant when stratified by vancomycin BMD MIC. There was no significant difference in the length of MRSA bacteremia. Variables independently associated with treatment failure included vancomycin therapy (adjusted odds ratio [aOR] = 2.16, 95% confidence interval [CI] = 1.24 to 3.76), intensive care unit admission (aOR = 2.46, 95% CI = 1.34 to 4.54), and infective endocarditis as the primary source (aOR = 2.33, 95% CI = 1.16 to 4.68). Treatment of MRSA BSIs with daptomycin was associated with reduced clinical failure and 30-day mortality; these findings were independent of vancomycin BMD MIC.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Sievert DM, Ricks P, Edwards JR, Schneider A, Patel J, Srinivasan A, Kallen A, Limbago B, Fridkin S, National Healthcare Safety Network (NHSN) Team and Participating NHSN Facilities. 2013. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009-2010. Infect Control Hosp Epidemiol 34:1–14. doi:10.1086/668770. - DOI - PubMed
-
- Bassetti M, Trecarichi EM, Mesini A, Spanu T, Giacobbe DR, Rossi M, Shenone E, Pascale GD, Molinari MP, Cauda R, Viscoli C, Tumbarello M. 2012. Risk factors and mortality of healthcare-associated and community-acquired Staphylococcus aureus bacteraemia. Clin Microbiol Infect 18:862–869. doi:10.1111/j.1469-0691.2011.03679.x. - DOI - PubMed
-
- Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak MJ, Talan DA, Chambers HF, Infectious Diseases Society of America. 2011. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis 52:e18–e55. doi:10.1093/cid/ciq146. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
