

The Shoulder Function Index (SFInX): evaluation of its measurement properties in people recovering from a proximal humeral fracture
- PMID: 27431393
- PMCID: PMC4950219
- DOI: 10.1186/s12891-016-1138-0
The Shoulder Function Index (SFInX): evaluation of its measurement properties in people recovering from a proximal humeral fracture
Abstract
Background: Concerns about test administration, reliability estimations, content and internal structure (dimensionality) of available shoulder measures for people with proximal humeral facture led to the development of a new clinician-observed outcome measure: the Shoulder Function Index (SFInX). The SFInX measures shoulder function by judgement of actual ability to perform daily tasks in which the shoulder is involved. Patients and health professionals had input into the instrument development, and Rasch analysis was used to create a unidimensional, interval-level scale. This study comprehensively evaluated the measurement properties of the SFInX in people recovering from a proximal humeral fracture.
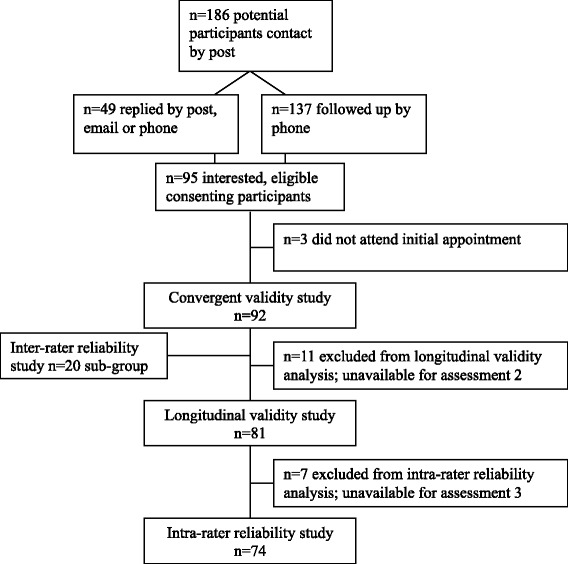
Methods: Data were collected on 92 people [79 women, mean age 63.5 years (SD13.9)] who sustained a proximal humeral fracture within the previous year on three occasions to allow for evaluation of the following measurement properties: construct validity (convergent, discriminant and known-groups validity), longitudinal validity (responsiveness), intra-rater reliability (one week retest interval), and inter-rater reliability (n = 20 subgroup; two independent raters). Comparative measures were Constant Score and Disabilities of the Arm Shoulder and Hand (DASH) and discriminative measure was a mental status questionnaire. Minimal clinically important difference, floor and ceiling effects and feasibility of the SFInX were also evaluated. A priori hypotheses were formulated where applicable.
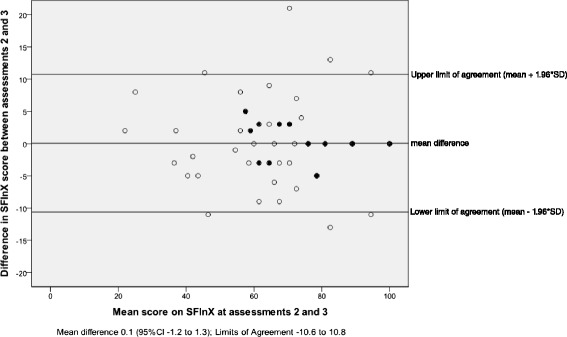
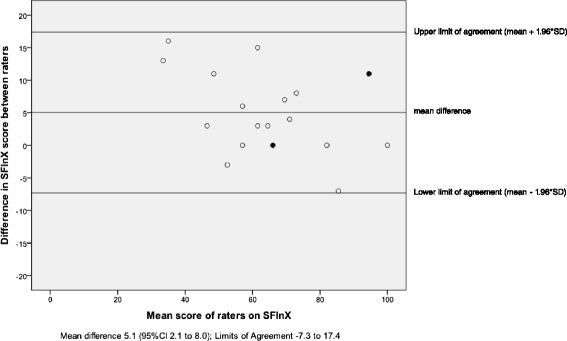
Results: Results for construct validity testing supported hypothesised relationships (convergent validity r = 0.75-0.89 (Constant Score and DASH); discriminant validity r = -0.08 (mental status); known-groups validity r = 0.50). For longitudinal validity, lower correlations (r = 0.40-0.49) than hypothesised (r = 0.50-0.70) were found. The SFInX scores changed more (10.3 points) than other scales, which could indicate that the SFInX is more responsive than the comparative measures. Intra-rater and inter-rater reliability found ICCs of 0.96 (95 % CI 0.94-0.97) and 0.91 (95 % CI 0.63-0.97) respectively, with low measurement error (SEM = 3.9-5.8/100). A change of 11-12 points (out of 100) was indicative of a clinically important difference.
Conclusions: The SFInX is a feasible outcome measure which clinicians can use to reliably measure and detect clinically important changes in the construct of 'shoulder function', the ability to perform activities in which the shoulder is involved, in people recovering from a proximal humeral fracture.
Keywords: Outcome Assessment (Health Care); Psychometrics; Rehabilitation; Reliability; Shoulder fractures; Shoulder function index; Validity.
Figures
Similar articles
-
The Shoulder Function Index (SFInX): a clinician-observed outcome measure for people with a proximal humeral fracture.BMC Musculoskelet Disord. 2015 Feb 18;16:31. doi: 10.1186/s12891-015-0481-x. BMC Musculoskelet Disord. 2015. PMID: 25887741 Free PMC article.
-
Reliability and validity of shoulder function outcome measures in people with a proximal humeral fracture.Disabil Rehabil. 2014;36(13):1072-9. doi: 10.3109/09638288.2013.829529. Epub 2013 Sep 3. Disabil Rehabil. 2014. PMID: 24001265
-
Reliability, validity, responsiveness, and minimal important change of the Disabilities of the Arm, Shoulder and Hand and Constant-Murley scores in patients with a humeral shaft fracture.J Shoulder Elbow Surg. 2017 Jan;26(1):e1-e12. doi: 10.1016/j.jse.2016.07.072. Epub 2016 Oct 10. J Shoulder Elbow Surg. 2017. PMID: 27745806
-
A Systematic Review and Standardized Comparison of Available Evidence for Outcome Measures Used to Evaluate Proximal Humerus Fracture Patients.J Orthop Trauma. 2019 Jul;33(7):e256-e262. doi: 10.1097/BOT.0000000000001462. J Orthop Trauma. 2019. PMID: 31135514
-
Psychometric Properties of Performance-Based Functional Tests in Patients With Shoulder Pathologies: A Systematic Review and Meta-analysis.Arch Phys Med Rehabil. 2020 Jun;101(6):1053-1063. doi: 10.1016/j.apmr.2019.11.011. Epub 2019 Dec 28. Arch Phys Med Rehabil. 2020. PMID: 31891713
Cited by
-
Fibula allograft in complex three-part and four-part proximal humeral fractures in active patients, a matched case-control study.JSES Int. 2023 Nov 17;8(1):21-26. doi: 10.1016/j.jseint.2023.10.004. eCollection 2024 Jan. JSES Int. 2023. PMID: 38312278 Free PMC article.
-
Shoulder Performance Activity Test (SPAT) for People With Shoulder Pain: Feasibility, Reliability, and Validity.Phys Ther. 2023 Mar 3;103(3):pzad006. doi: 10.1093/ptj/pzad006. Phys Ther. 2023. PMID: 37172131 Free PMC article.
-
Psychometric properties of patient-reported outcomes measures used to assess upper limb pathology: a systematic review.ANZ J Surg. 2022 Dec;92(12):3170-3175. doi: 10.1111/ans.17973. Epub 2022 Aug 12. ANZ J Surg. 2022. PMID: 35959939 Free PMC article.
-
How to Assess Shoulder Functionality: A Systematic Review of Existing Validated Outcome Measures.Diagnostics (Basel). 2021 May 8;11(5):845. doi: 10.3390/diagnostics11050845. Diagnostics (Basel). 2021. PMID: 34066777 Free PMC article. Review.
-
Humeral Head Replacement in the Treatment of Comminuted Proximal Humeral Fracture.Orthop Surg. 2021 Feb;13(1):28-34. doi: 10.1111/os.12732. Epub 2021 Jan 5. Orthop Surg. 2021. PMID: 33403829 Free PMC article.
References
-
- Ismail AA, Pye SR, Cockerill WC, Lunt M, Silman AJ, Reeve J, Banzer D, Benevolenskaya LI, Bhalla A, Bruges Armas J, et al. Incidence of limb fracture across Europe: results from the European Prospective Osteoporosis Study (EPOS) Osteoporos Int. 2002;13(7):565–571. doi: 10.1007/s001980200074. - DOI - PubMed
-
- Olerud P, Ahrengart L, Söderqvist A, Saving J, Tidermark J. Quality of life and functional outcome after a 2- part proximal humeral fracture: A prospective cohort study on 50 patients treated with a locking plate. J Shoulder Elbow Surg. 2010;19(6):814-22. doi:10.1016/j.jse.2009.11.046. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
