

Development of a risk prediction model for transfusion in carotid endarterectomy and demonstration of cost-saving potential by avoidance of "type and screen"
- PMID: 27432200
- PMCID: PMC5121067
- DOI: 10.1016/j.jvs.2016.04.059
Development of a risk prediction model for transfusion in carotid endarterectomy and demonstration of cost-saving potential by avoidance of "type and screen"
Abstract
Objective: Preoperative testing for carotid endarterectomy (CEA) often includes blood typing and antibody screen (T&S). In our institutional experience, however, transfusion for CEA is rare. We assessed transfusion rate and risk factors in a national clinical database to identify a cohort of patients in whom T&S can safely be avoided with the potential for substantial cost savings.
Methods: With use of the National Surgical Quality Improvement Program database, transfusion events and timing were established for all elective CEAs in 2012-2013. Comorbidities and other characteristics were compared for patients receiving intraoperative or postoperative transfusion and those who did not. After random assignment of the total data to either a training or validation set, a prediction model for transfusion risk was created and subsequently validated.
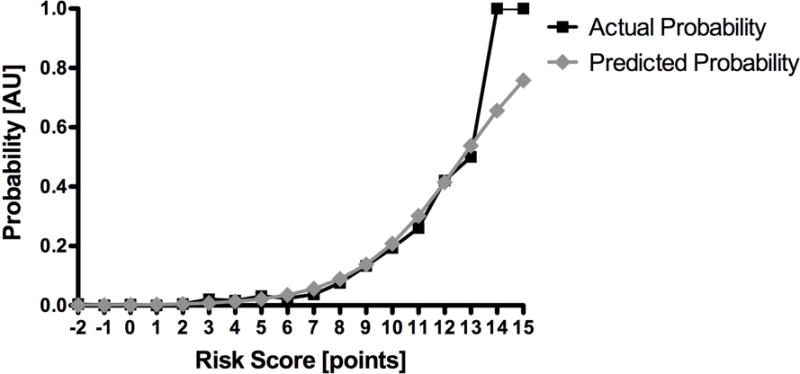
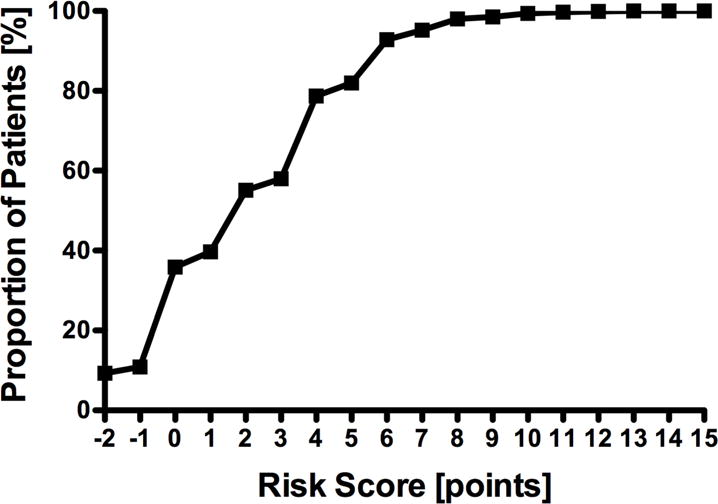
Results: Of 16,043 patients undergoing CEA in 2012-2013, 276 received at least one transfusion before discharge (1.7%); 42% of transfusions occurred on the day of surgery. Preoperative hematocrit <30% (odds ratio [OR], 57.4; 95% confidence interval [CI], 29.6-111.1), history of congestive heart failure (OR, 2.8; 95% CI, 1.1-7.1), dependent functional status (OR, 2.7; 95% CI, 1.5-5.1), coagulopathy (OR, 2.5; 95% CI, 1.7-3.6), creatinine concentration ≥1.2 mg/dL (OR, 2.3; 95% CI, 1.6-3.3), preoperative dyspnea (OR, 2.0; 95% CI, 1.4-3.1), and female gender (OR, 1.6; 95% CI, 1.1-2.3) predicted transfusion. A risk prediction model based on these data produced a C statistic of 0.85; application of this model to the validation set demonstrated a C statistic of 0.81. In the validation set, 93% of patients received a score of 6 or less, corresponding to an individual predicted transfusion risk of 5% or less. Omitting a T&S in these patients would generate a substantial annual cost saving for National Surgical Quality Improvement Program hospitals.
Conclusions: Whereas T&S are commonly performed for patients undergoing CEA, transfusion after CEA is rare and well predicted by a transfusion risk score. Avoidance of T&S in this low-risk population provides a substantial cost-saving opportunity without compromise of patient care.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Donati A. A new and feasible model for predicting operative risk. Br J Anaesth. 2004 Sep 1;93(3):393–399. - PubMed
-
- Carson JL, Duff A, Poses RM, Berlin JA, Spence RK, Trout R, et al. Effect of anaemia and cardiovascular disease on surgical mortality and morbidity. The Lancet. 1996 Oct;348(9034):1055–1060. - PubMed
-
- Hobson RW, Weiss DG, Fields WS, Goldstone J, Moore WS, Towne JB, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med. 1993 Jan 28;328(4):221–227. - PubMed
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug 15;325(7):445–453. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
