

DNA Mismatch Repair Deficiency in Rectal Cancer: Benchmarking Its Impact on Prognosis, Neoadjuvant Response Prediction, and Clinical Cancer Genetics
- PMID: 27432916
- PMCID: PMC5012714
- DOI: 10.1200/JCO.2016.66.6826
DNA Mismatch Repair Deficiency in Rectal Cancer: Benchmarking Its Impact on Prognosis, Neoadjuvant Response Prediction, and Clinical Cancer Genetics
Abstract
Purpose: DNA mismatch repair deficiency (dMMR) hallmarks consensus molecular subtype 1 of colorectal cancer. It is being routinely tested, but little is known about dMMR rectal cancers. The efficacy of novel treatment strategies cannot be established without benchmarking the outcomes of dMMR rectal cancer with current therapy. We aimed to delineate the impact of dMMR on prognosis, the predicted response to fluoropyrimidine-based neoadjuvant therapy, and implications of germline alterations in the MMR genes in rectal cancer.
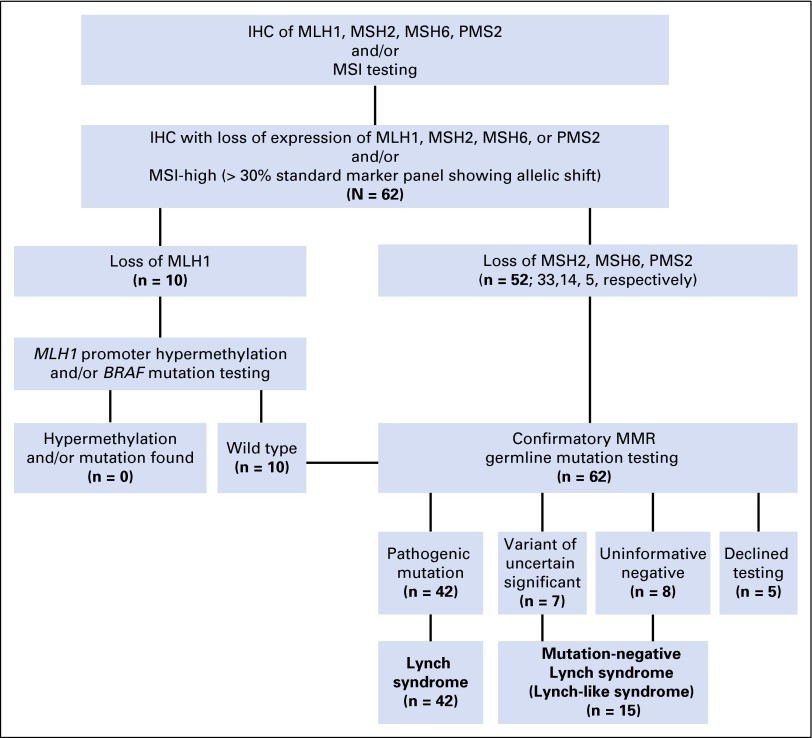
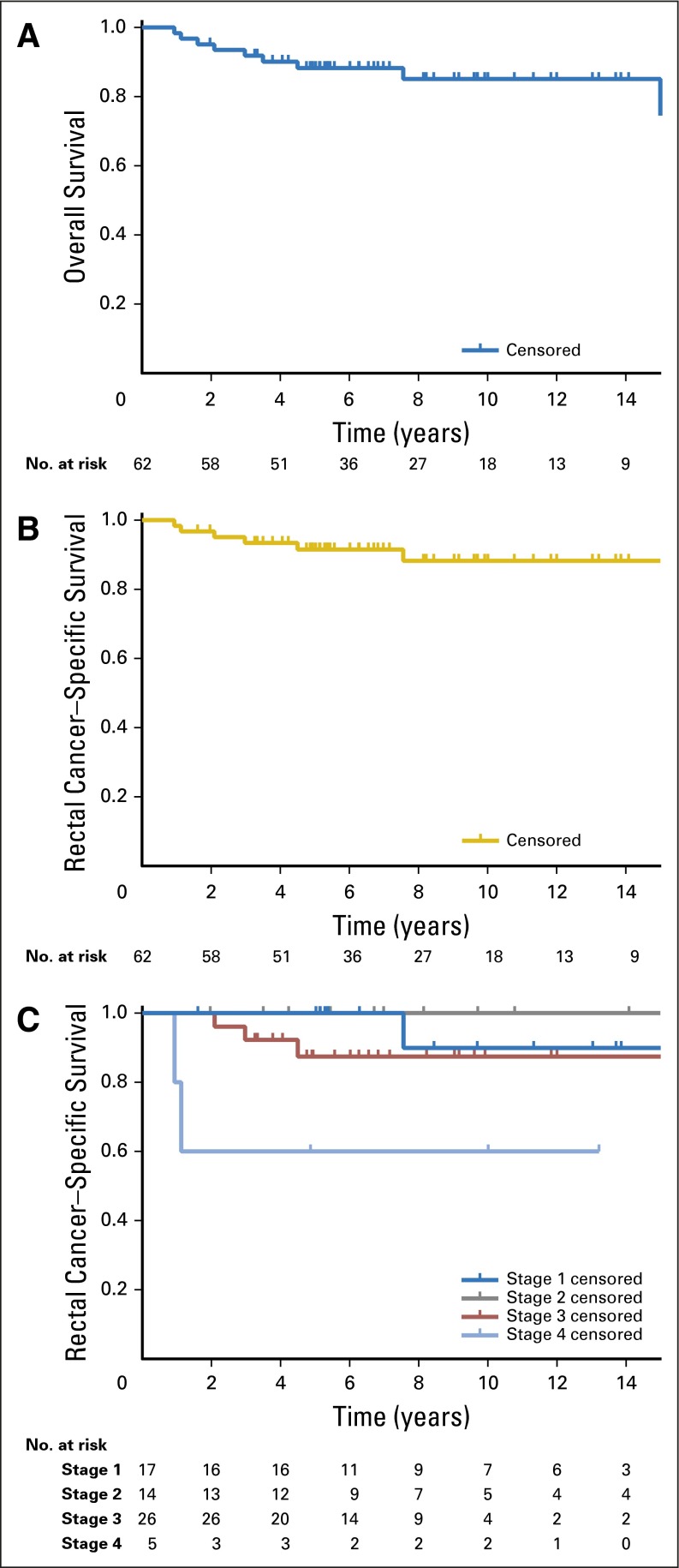
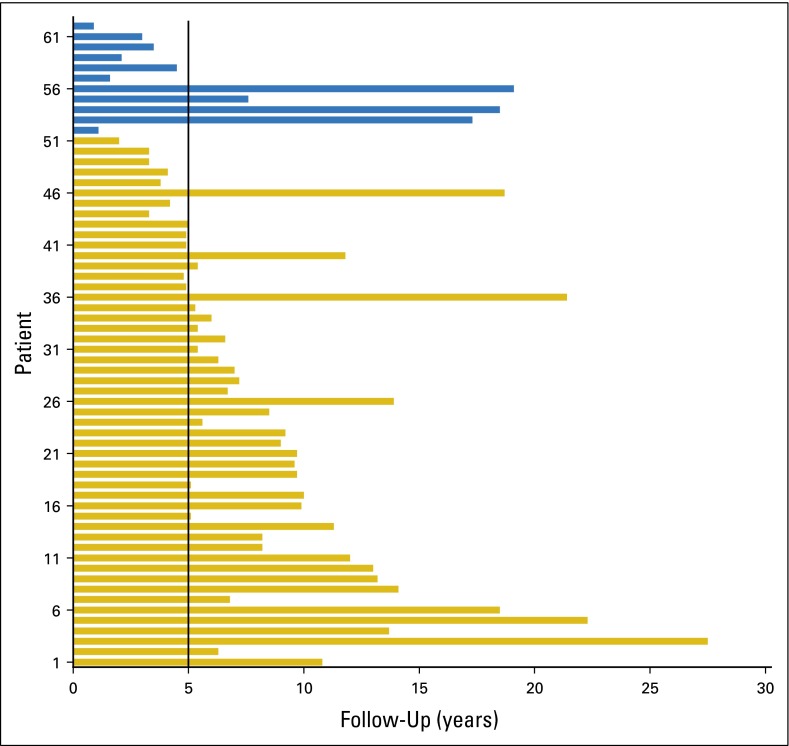
Methods: Between 1992 and 2012, 62 patients with dMMR rectal cancers underwent multimodality therapy. Oncologic treatment and outcomes as well as clinical genetics work-up were examined. Overall and rectal cancer-specific survival were calculated by the Kaplan-Meier method.
Results: The median age at diagnosis was 41 years. MMR deficiency was most commonly due to alterations in MSH2 (53%) or MSH6 (23%). After a median follow-up of 6.8 years, the 5-year rectal cancer-specific survival was 100% for stage I and II, 85.1% for stage III, and 60.0% for stage IV disease. Fluoropyrimidine-based neoadjuvant chemoradiation was associated with a complete pathologic response rate of 27.6%. The extent of surgical resection was influenced by synchronous colonic disease at presentation, tumor height, clinical stage, and pelvic radiation. An informed decision for a limited resection focusing on proctectomy did not compromise overall survival. Five of the 11 (45.5%) deaths during follow-up were due to extracolorectal malignancies.
Conclusion: dMMR rectal cancer had excellent prognosis and pathologic response with current multimodality therapy including an individualized surgical treatment plan. Identification of a dMMR rectal cancer should trigger germline testing, followed by lifelong surveillance for both colorectal and extracolorectal malignancies. We herein provide genotype-specific outcome benchmarks for comparison with novel interventions.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Similar articles
-
Mismatch Repair-Deficient Rectal Cancer and Resistance to Neoadjuvant Chemotherapy.Clin Cancer Res. 2020 Jul 1;26(13):3271-3279. doi: 10.1158/1078-0432.CCR-19-3728. Epub 2020 Mar 6. Clin Cancer Res. 2020. PMID: 32144135 Free PMC article.
-
Incidence and Outcomes of Patients With Mismatch Repair Deficient Rectal Cancer Operated in 2016: A Nationwide Cohort From The Netherlands.Clin Colorectal Cancer. 2025 Jun;24(2):188-197.e1. doi: 10.1016/j.clcc.2024.12.003. Epub 2024 Dec 10. Clin Colorectal Cancer. 2025. PMID: 39741022
-
Mismatch Repair System Deficiency Is Associated With Response to Neoadjuvant Chemoradiation in Locally Advanced Rectal Cancer.Int J Radiat Oncol Biol Phys. 2019 Nov 15;105(4):824-833. doi: 10.1016/j.ijrobp.2019.07.057. Epub 2019 Aug 9. Int J Radiat Oncol Biol Phys. 2019. PMID: 31404579
-
Microsatellite instability testing and its role in the management of colorectal cancer.Curr Treat Options Oncol. 2015 Jul;16(7):30. doi: 10.1007/s11864-015-0348-2. Curr Treat Options Oncol. 2015. PMID: 26031544 Free PMC article. Review.
-
Preoperative Strategies for Locally Advanced Colon Cancer.Curr Treat Options Oncol. 2024 Mar;25(3):376-388. doi: 10.1007/s11864-024-01184-6. Epub 2024 Feb 13. Curr Treat Options Oncol. 2024. PMID: 38349502 Free PMC article. Review.
Cited by
-
Efficacy and safety-in analysis of short-course radiation followed by mFOLFOX-6 plus avelumab for locally advanced rectal adenocarcinoma.Radiat Oncol. 2020 Oct 7;15(1):233. doi: 10.1186/s13014-020-01673-6. Radiat Oncol. 2020. PMID: 33028346 Free PMC article. Clinical Trial.
-
Mismatch repair protein expression and intratumoral budding in rectal cancer are associated with an increased pathological complete response to preoperative chemoradiotherapy: A case-control study.World J Clin Oncol. 2018 Nov 10;9(7):133-139. doi: 10.5306/wjco.v9.i7.133. World J Clin Oncol. 2018. PMID: 30425938 Free PMC article.
-
Developments in Checkpoint Inhibitor Therapy for the Management of Deficient Mismatch Repair (dMMR) Rectal Cancer.Curr Oncol. 2023 Mar 26;30(4):3672-3683. doi: 10.3390/curroncol30040279. Curr Oncol. 2023. PMID: 37185392 Free PMC article. Review.
-
Evaluation of Changes in Circulating Cell-Free DNA as an Early Predictor of Response to Chemoradiation in Rectal Cancer-A Pilot Study.Medicina (Kaunas). 2023 Sep 28;59(10):1742. doi: 10.3390/medicina59101742. Medicina (Kaunas). 2023. PMID: 37893461 Free PMC article.
-
Can Microsatellite Status of Colorectal Cancer Be Reliably Assessed after Neoadjuvant Therapy?Clin Cancer Res. 2017 Sep 1;23(17):5246-5254. doi: 10.1158/1078-0432.CCR-16-2994. Epub 2017 May 18. Clin Cancer Res. 2017. PMID: 28522602 Free PMC article.
References
-
- Stoffel EM, Mangu PB, Gruber SB, et al. Hereditary colorectal cancer syndromes: American Society of Clinical Oncology Clinical Practice Guideline endorsement of the familial risk-colorectal cancer: European Society for Medical Oncology Clinical Practice Guidelines. J Clin Oncol. 2015;33:209–217. - PMC - PubMed
-
- Weissman SM, Burt R, Church J, et al. Identification of individuals at risk for Lynch syndrome using targeted evaluations and genetic testing: National Society of Genetic Counselors and the Collaborative Group of the Americas on Inherited Colorectal Cancer joint practice guideline. J Genet Couns. 2012;21:484–493. - PubMed
-
- Hampel H. Point: Justification for Lynch syndrome screening among all patients with newly diagnosed colorectal cancer. J Natl Compr Canc Netw. 2010;8:597–601. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
