

Nationwide trends and predictors of inpatient mortality in 83884 transjugular intrahepatic portosystemic shunt
- PMID: 27433091
- PMCID: PMC4932213
- DOI: 10.3748/wjg.v22.i25.5780
Nationwide trends and predictors of inpatient mortality in 83884 transjugular intrahepatic portosystemic shunt
Abstract
Aim: To evaluate and validate the national trends and predictors of in-patient mortality of transjugular intrahepatic portosystemic shunt (TIPS) in 15 years.
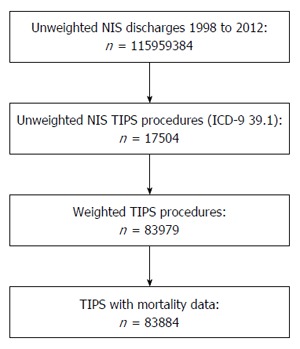
Methods: Using the National Inpatient Sample which is a part of Health Cost and Utilization Project, we identified a discharge-weighted national estimate of 83884 TIPS procedures performed in the United States from 1998 to 2012 using international classification of diseases-9 procedural code 39.1. The demographic, hospital and co-morbility data were analyzed using a multivariant analysis. Using multi-nominal logistic regression analysis, we determined predictive factors related to increases in-hospital mortality. Comorbidity measures are in accordance to the Comorbidity Software designed by the Agency for Healthcare Research and Quality.
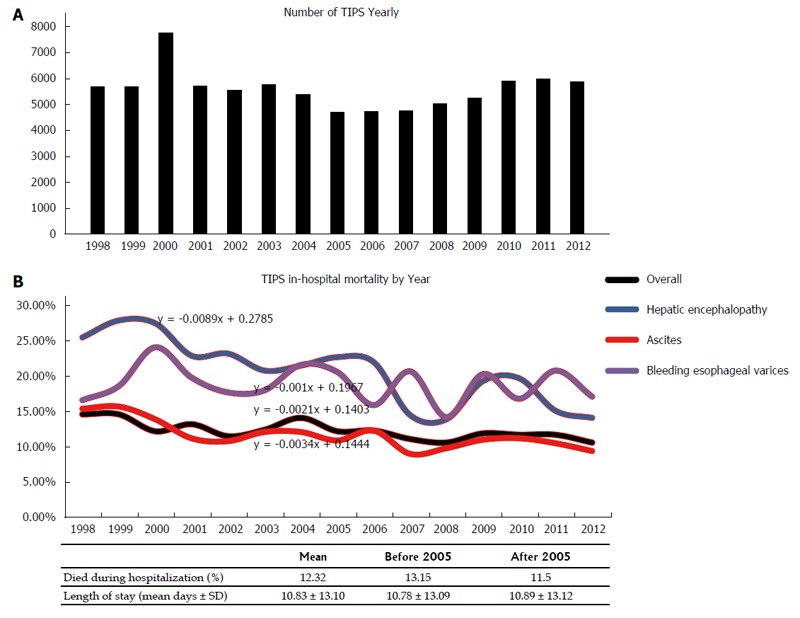
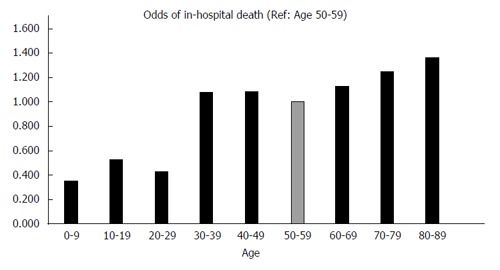
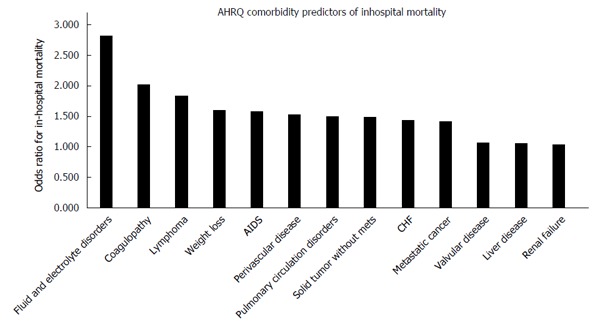
Results: Overall, 12.3% of patients died during hospitalization with downward trend in-hospital mortality with the mean length of stay of 10.8 ± 13.1 d. Notable, African American patients (OR = 1.809 vs Caucasian patients, P < 0.001), transferred patients (OR = 1.347 vs non-transferred, P < 0.001), emergency admissions (OR = 3.032 vs elective cases, P < 0.001), patients in the Northeast region (OR = 1.449 vs West, P < 0.001) had significantly higher odds of in-hospital mortality. Number of diagnoses and number of procedures showed positive correlations with in-hospital death (OR = 1.249 per one increase in number of procedures). Patients diagnosed with acute respiratory failure (OR = 8.246), acute kidney failure (OR = 4.359), hepatic encephalopathy (OR = 2.217) and esophageal variceal bleeding (OR = 2.187) were at considerably higher odds of in-hospital death compared with ascites (OR = 0.136, P < 0.001). Comorbidity measures with the highest odds of in-hospital death were fluid and electrolyte disorders (OR = 2.823), coagulopathy (OR = 2.016), and lymphoma (OR = 1.842).
Conclusion: The overall mortality of the TIPS procedure is steadily decreasing, though the length of stay has remained relatively constant. Specific patient ethnicity, location, transfer status, primary diagnosis and comorbidities correlate with increased odds of TIPS in-hospital death.
Keywords: Health Cost and Utilization Project; Inpatient; Mortality; National Inpatient Sample database; Transjugular intrahepatic portosystemic shunt; United States.
Figures
References
-
- Boyer TD, Haskal ZJ. The Role of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in the Management of Portal Hypertension: update 2009. Hepatology. 2010;51:306. - PubMed
-
- Yang Z, Han G, Wu Q, Ye X, Jin Z, Yin Z, Qi X, Bai M, Wu K, Fan D. Patency and clinical outcomes of transjugular intrahepatic portosystemic shunt with polytetrafluoroethylene-covered stents versus bare stents: a meta-analysis. J Gastroenterol Hepatol. 2010;25:1718–1725. - PubMed
-
- Quiroga J, Sangro B, Núñez M, Bilbao I, Longo J, García-Villarreal L, Zozaya JM, Betés M, Herrero JI, Prieto J. Transjugular intrahepatic portal-systemic shunt in the treatment of refractory ascites: effect on clinical, renal, humoral, and hemodynamic parameters. Hepatology. 1995;21:986–994. - PubMed
-
- Ferral H, Gamboa P, Postoak DW, Albernaz VS, Young CR, Speeg KV, McMahan CA. Survival after elective transjugular intrahepatic portosystemic shunt creation: prediction with model for end-stage liver disease score. Radiology. 2004;231:231–236. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
