

Can ultrasound help to manage patients with scrotal trauma?
- PMID: 27433221
- PMCID: PMC4760557
- DOI: 10.1177/1742271X14545911
Can ultrasound help to manage patients with scrotal trauma?
Abstract
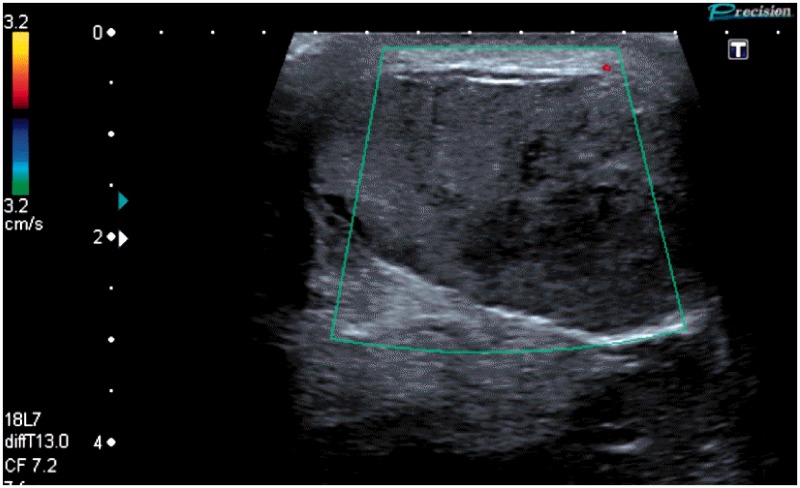
Traumatic injuries to the scrotum are uncommon but, when they do occur, frequently lead to serious complications. Early complications include testicular infarction, necrosis and abscess formation; in the longer-term trauma may result in testicular atrophy and subfertility. Early surgical intervention in patients with testicular rupture can significantly improve the clinical outcome and reduce the need for delayed orchidectomy. However, clinical examination of the scrotum following trauma is difficult and frequently inaccurate; this may result in incorrect triage of patients for surgical exploration. Scrotal ultrasound can reliably assess scrotal injuries and diagnose testicular rupture with a high level of accuracy. Additionally, ultrasound can provide important information regarding testicular perfusion, which can further inform decisions on surgical management. This article reviews the sonographic findings that may be encountered in patients with scrotal trauma, with an emphasis on blunt trauma. It describes the pivotal role that ultrasound can play in the accurate triage of these patients to surgical or conservative management.
Keywords: Ultrasound testis; testicular rupture; testicular trauma; ultrasound scrotum.
Figures









References
-
- Munter DW, Faleski EJ. Blunt scrotal trauma: emergency department evaluation and management. Am J Emerg Med 1989; 7: 227–34. - PubMed
-
- Cross JJL, Berman LH, Elliott PG, Irving S. Scrotal trauma: a cause of testicular atrophy. Clin Radiol 1999; 54: 317–20. - PubMed
-
- Kukadia AN, Ercole CJ, Gleich P, Hensleigh H, Pryor JL. Testicular trauma: potential impact on reproductive function. J Urol 1996; 156: 1643–6. - PubMed
-
- Lin WW, Kim ED, Quesada ET, Lipshultz LI, Coburn M. Unilateral testicular injury from external trauma: evaluation of semen quality and endocrine parameters. J Urol 1998; 159: 841–3. - PubMed
-
- Chandra RV, Dowling RJ, Ulubasoglu M, Haxhimolla H, Costello AJ. Rational approach to diagnosis and management of blunt scrotal trauma. Urology 2007; 70: 230–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources