

Review
doi: 10.1177/1742271X15588809.
Epub 2015 Jun 11.
Ultrasound of lower limb sports injuries
Affiliations
- PMID: 27433251
- PMCID: PMC4760585
- DOI: 10.1177/1742271X15588809
Item in Clipboard
Review
Ultrasound of lower limb sports injuries
Ultrasound.
2015 Aug.
Abstract
Musculoskeletal ultrasound utilises high-frequency linear transducers to produce high-resolution images of soft tissue structures. It is an increasingly useful tool in the assessment of both acute and chronic musculoskeletal injuries; it is relatively cheap, portable and can be used to facilitate targeted injections. In this review paper, we aim to provide a summary on the normal and abnormal appearances of skeletal tissue in the setting of acute and chronic lower limb sporting injuries.
Keywords: Ultrasound; injuries; lower limb; sports.
Figures
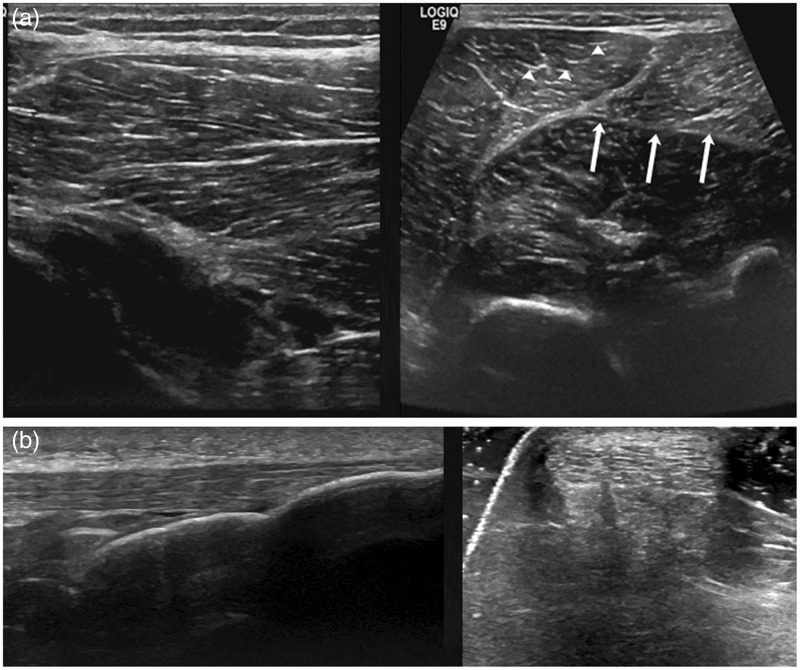
(a) Longitudinal and transverse views of normal skeletal muscle. The arrow heads show innumerable hyperechoic dots/dashes, which represent the perimysium. The epimysium (arrows) demarcates the hyperechoic fascial boundary surrounding the muscle. (b) Longitudinal and transverse views of a normal Achilles tendon. Normal tendon appears as an array of echogenic parallel lines (bundles of collagen fibres) or as multiple echogenic dots on short axis
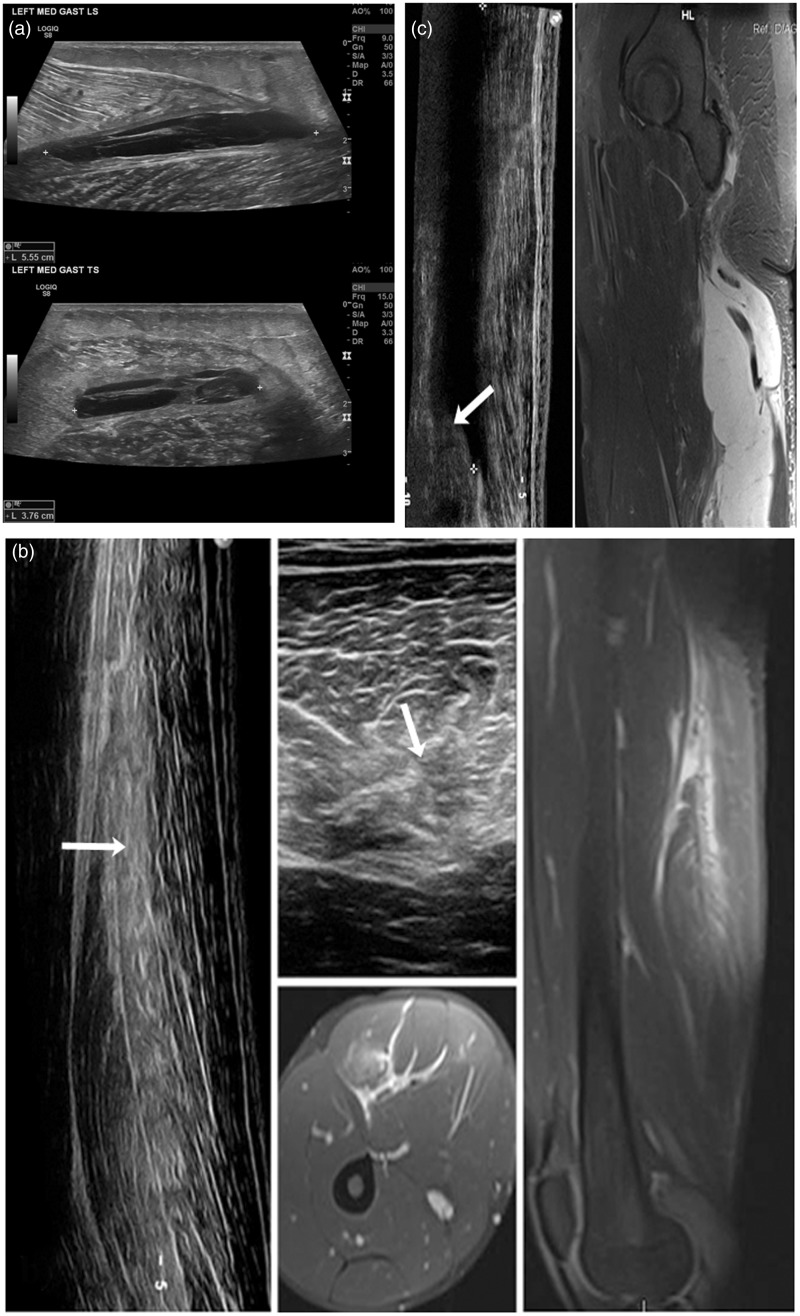
(a) Longitudinal and transverse views of the left gastrocnemius muscle in a female runner showing a 5.5 cm myofascial separation tear consistent with a grade II injury. Complexity and stranding within the hypoechoic area represents blood clot. Intact muscle fibres are seen on the transverse view. (b) Longitudinal and transverse views of the hamstring muscle in a footballer demonstrating moderately extensive hyperechoic change representing haemorrhage and oedema (white arrow) suggestive of a grade II injury. Contemporaneous MRI images of the same injury show a small discrete haematoma and muscle fibre retraction. (c) A longitudinal view of the hamstrings in a water skier with a corresponding MRI image. The white arrow demonstrates the proximal end of the retracted muscle stump consistent with a grade III injury
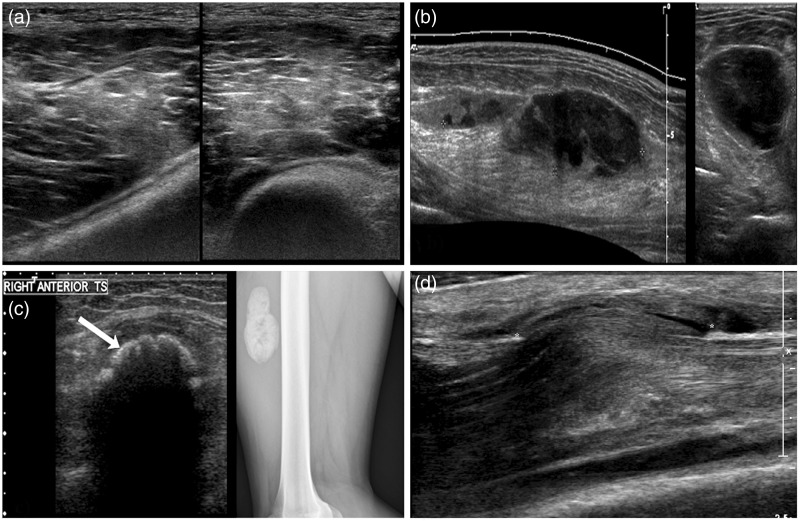
(a) Longitudinal and transverse views of the vastus medialis obliquus muscle following blunt direct trauma. Diffuse hyperechoic change and loss of fibrillar architecture represents acute bleeding and oedema within the muscle with no loss of continuity. (b) Longitudinal and transverse views of a 9 cm calf haematoma following direct trauma. This may evolve into a more hypoechoic looking seroma which may be amenable to aspiration to expedite recovery. (c) Transverse view of the anterior thigh in a footballer 3 months post blunt trauma. A highly reflective curvilinear opacity within the muscle substance (white arrow) casting dense posterior acoustic shadowing. The corresponding lateral radiograph shows a smooth lobular calcified mass lying anterior to the femoral cortex, consistent with myositis ossificans. (d) An acute muscle hernia in a professional footballer following blunt trauma. Bulging of the tibialis anterior muscle through a defect in the overlying fascia (*) is shown with adjacent haemorrhage
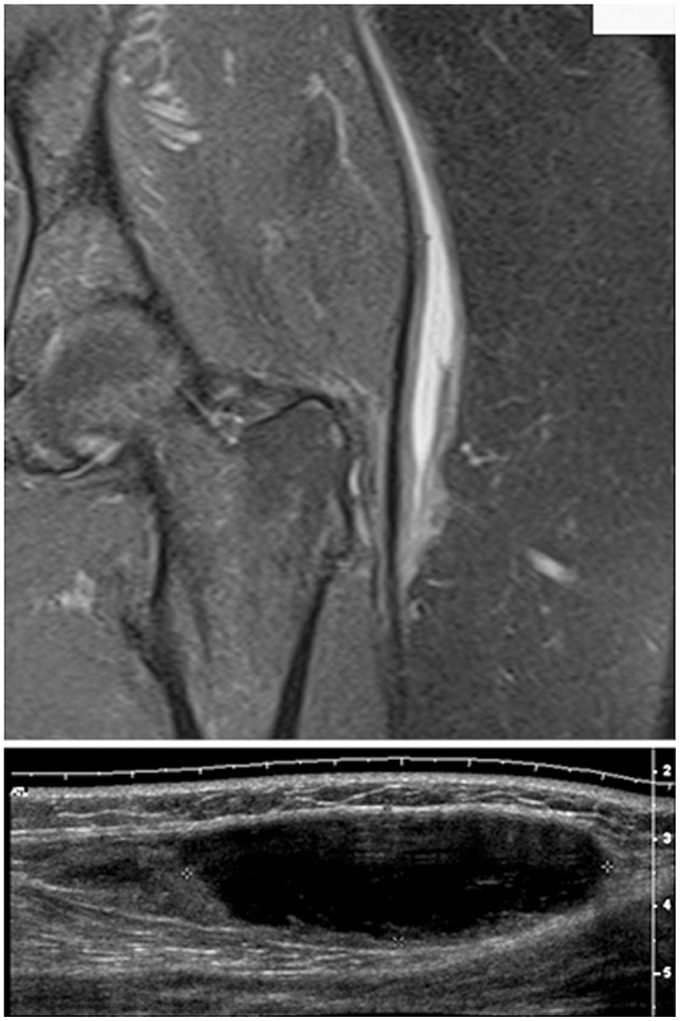
A coronal fluid sensitive MRI image and a longitudinal ultrasound view, in different patients, showing a pocket of serous fluid lying at the junction of the subcutaneous fat and underlying fascia lata. Often from blunt trauma, the subcutaneous fat sheers off from the underling fascia creating a potential space
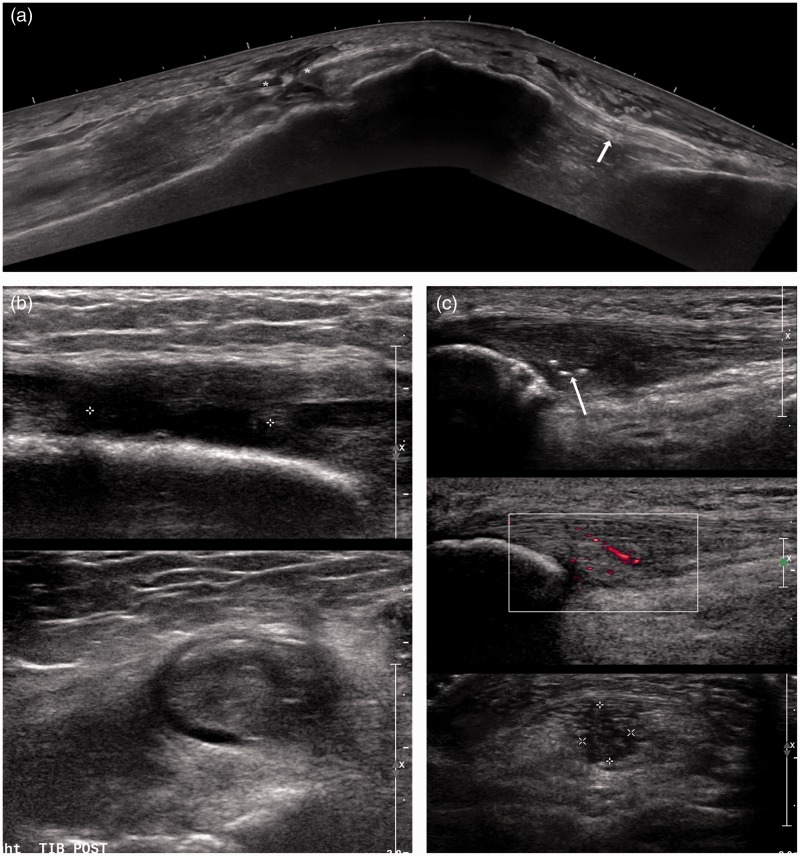
(a) A panoramic longitudinal view of the extensor mechanism in a middle aged man showing a complete full thickness rupture of the central fibres of the quadriceps tendon. Intact tendon fibres of vastus lateralis were seen. The partially retracted tendon ends are shown (*). Normal fibrillar structure of the patellar tendon is demonstrated (white arrow). (b) Longitudinal and transverse views of the right tibialis posterior tendon. There is complete loss of continuity (grade III) of the tendon with hypoechoic fluid seen within the tendon sheath. (c) Longitudinal and transverse views of the proximal patellar tendon showing thickening, hypoechoic change, and loss of fibrillar architecture. Focal areas of dystrophic calcification represented by three echogenic foci are also present (white arrow). Appearances are consistent with chronic patellar tendinosis with neovascularity within the proximal patellar tendon
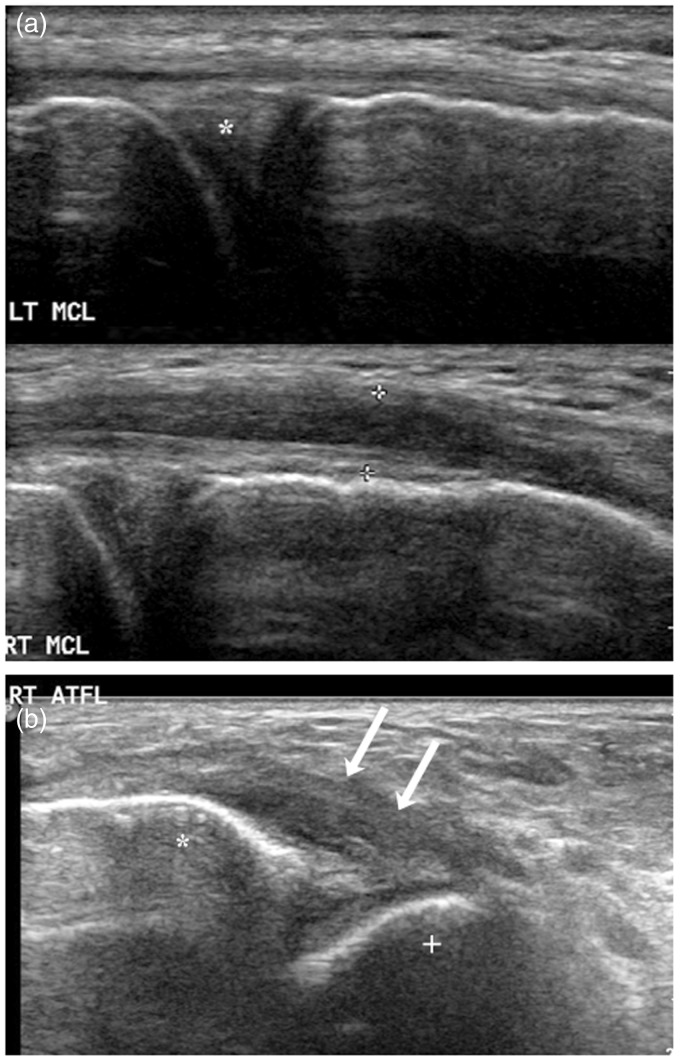
(a) A longitudinal view of a normal left MCL which appears thin with preserved fibrillar architecture. In comparison, a longitudinal view of an injured right MCL which is thickened and hypoechoic but remains intact (grade II injury). The medial joint space and medial meniscus (*) are seen deep to the MCL. (b) The white arrows demonstrate grossly thickening hypoechoic change to the right anterior talofibular ligament following an inversion injury consistent with an acute grade II injury (* = fibular; + = talus)
Similar articles
-
A one-stop approach to the management of soft tissue and degenerative musculoskeletal conditions using clinic-based ultrasonography.Musculoskeletal Care. 2011 Jun;9(2):63-8. doi: 10.1002/msc.194. Epub 2010 Nov 2. Musculoskeletal Care. 2011. PMID: 21618397
-
Musculoskeletal Simulation Tools for Understanding Mechanisms of Lower-Limb Sports Injuries.Curr Sports Med Rep. 2019 Jun;18(6):210-216. doi: 10.1249/JSR.0000000000000601. Curr Sports Med Rep. 2019. PMID: 31385836 Review.
-
The application of musculoskeletal ultrasonography in sports injuries of lower limbs in Chongqing Marathon competition.J Sports Med Phys Fitness. 2020 Jan;60(1):102-109. doi: 10.23736/S0022-4707.19.09925-0. Epub 2019 Dec 5. J Sports Med Phys Fitness. 2020. PMID: 31818053
-
Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes.J Phys Ther Sci. 2017 Jan;29(1):12-15. doi: 10.1589/jpts.29.12. Epub 2017 Jan 30. J Phys Ther Sci. 2017. PMID: 28210029 Free PMC article.
-
Introduction to diagnostic musculoskeletal ultrasound: part 2: examination of the lower limb.Am J Phys Med Rehabil. 2008 Mar;87(3):238-48. doi: 10.1097/PHM.0b013e31816198c2. Am J Phys Med Rehabil. 2008. PMID: 18174843 Review.
Cited by
-
Intra-session and inter-rater reliability of spatial frequency analysis methods in skeletal muscle.PLoS One. 2020 Jul 10;15(7):e0235924. doi: 10.1371/journal.pone.0235924. eCollection 2020. PLoS One. 2020. PMID: 32649705 Free PMC article.
-
The popliteofibular ligament: a cadaveric ultrasound study.Skeletal Radiol. 2022 Jan;51(1):183-189. doi: 10.1007/s00256-021-03813-9. Epub 2021 Jun 19. Skeletal Radiol. 2022. PMID: 34146118 Free PMC article.
-
Ultrasound Imaging in Diagnosis and Management of Lower Limb Injuries: A Comprehensive Review.Med Sci Monit. 2024 Sep 3;30:e945413. doi: 10.12659/MSM.945413. Med Sci Monit. 2024. PMID: 39223775 Free PMC article. Review.
-
Use of Reflective Tape to Detect Ultrasound Transducer Movement: A Validation Study.Life (Basel). 2021 Jan 30;11(2):104. doi: 10.3390/life11020104. Life (Basel). 2021. PMID: 33573159 Free PMC article.
References
-
- Weatherall PT, Crues JV. Musculotendinous injury. Magn Reson Imaging Clin N Am 1995; 3: 753–72. - PubMed
-
- Torriani M, Kattapuram SV. Musculoskeletal ultrasound: an alternative imaging modality for sports-related injuries. Top Magn Reson Imaging 2003; 14: 103–111. - PubMed
-
- Erickson SJ. Sonography of the foot and ankle. Foot Ankle Clin 2000; 5: 29–48 (v). - PubMed
Publication types
LinkOut - more resources
Full Text Sources