

MASTERS-D Study: A Prospective, Multicenter, Pragmatic, Observational, Data-Monitored Trial of Minimally Invasive Fusion to Treat Degenerative Lumbar Disorders, One-Year Follow-Up
- PMID: 27433419
- PMCID: PMC4945329
- DOI: 10.7759/cureus.640
MASTERS-D Study: A Prospective, Multicenter, Pragmatic, Observational, Data-Monitored Trial of Minimally Invasive Fusion to Treat Degenerative Lumbar Disorders, One-Year Follow-Up
Abstract
The objective of the study is to assess effectiveness and safety of minimally invasive lumbar interbody fusion (MILIF) for degenerative lumbar disorders (DLD) in daily surgical practice and follow up with patients for one year after surgery. A prospective, multicenter, pragmatic, monitored, international outcome study in patients with DLD causing back/leg pain was conducted (19 centers). Two hundred fifty-two patients received standard of care available in the centers. Patients were included if they were aged >18 years, required one- or two-level lumbar fusion for DLD, and met the criteria for approved device indications. Primary endpoints: time to first ambulation (TFA) and time to surgery recovery (TSR). Secondary endpoints: patient-reported outcomes (PROs)--back and leg pain (visual analog scale), disability (Oswestry Disability Index (ODI)), health status (EQ-5D), fusion rates, reoperation rates, change in pain medication, rehabilitation, return to work, patient satisfaction, and adverse events (AEs). Experienced surgeons (≥30 surgeries pre-study) treated patients with DLD by one- or two-level MILIF and patients were evaluated for one year (NCT01143324). At one year, 92% (233/252) of patients remained in the study.
Primary outcomes: TFA, 1.3 ±0.5 days and TSR, 3.2 ±2.0 days.
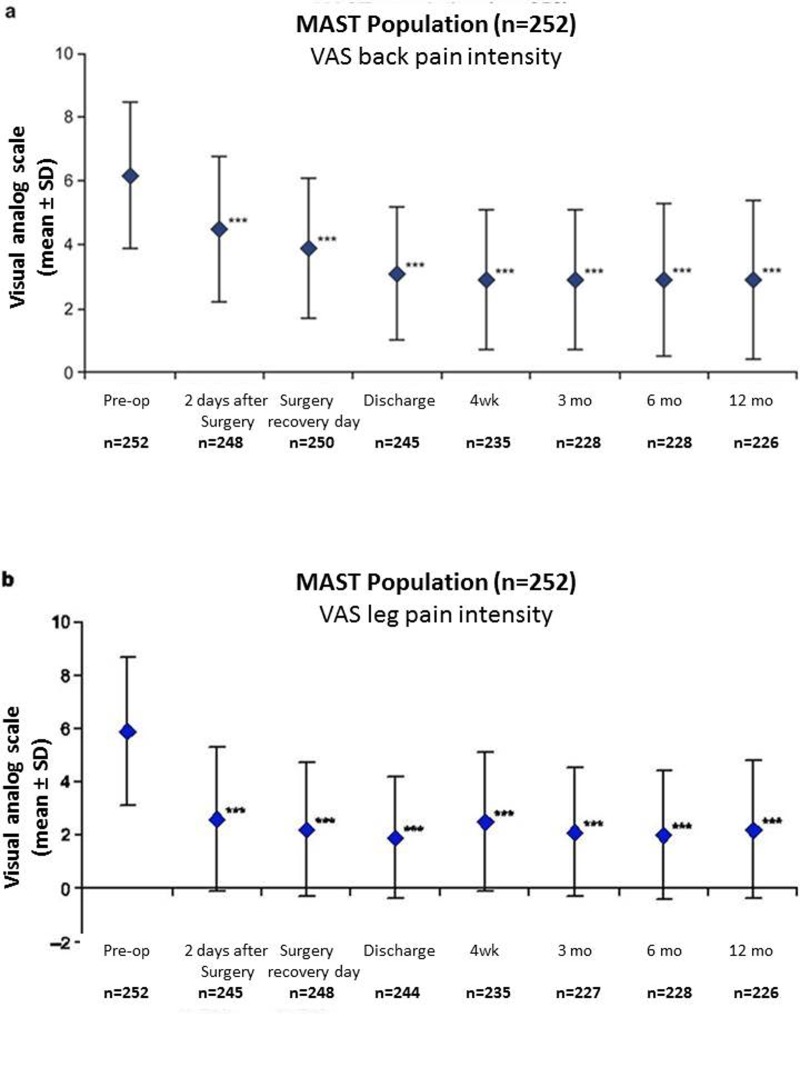
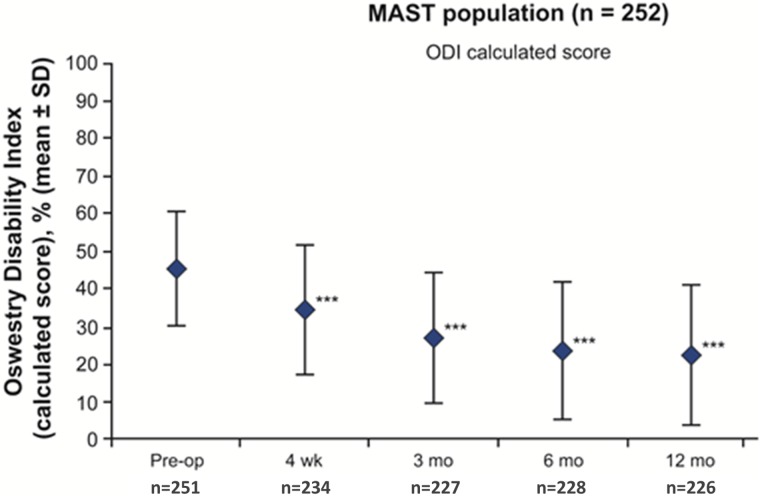
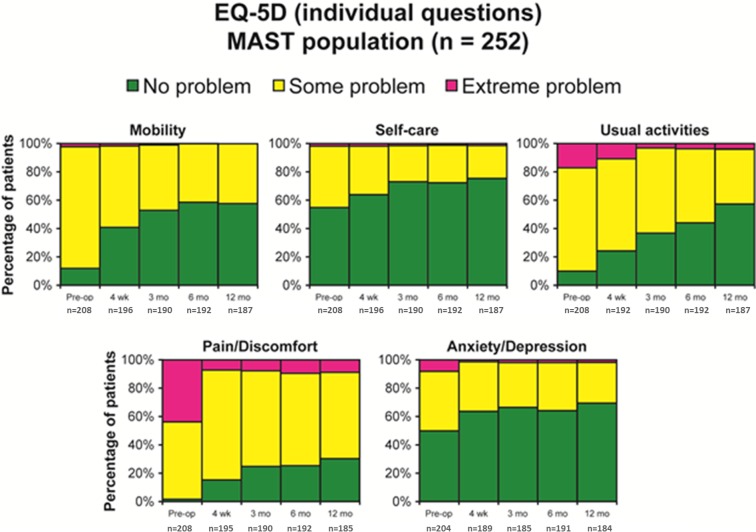
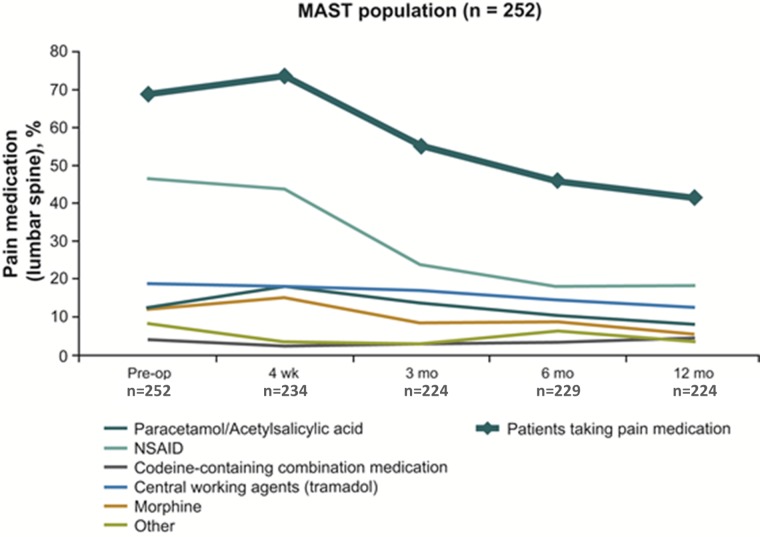
Secondary outcomes: Most patients (83.3%) received one level MILIF; one (two-level) MILIF mean surgery duration, 128 (182) min; fluoroscopy time, 115 (154) sec; blood loss, 164 (233) mL; at one year statistically significant (P<.0001) and clinically meaningful changes from baseline were reported in all PROs--reduced back pain (2.9 ±2.5 vs. 6.2 ±2.3 at intake), reduced leg pain (2.2 ±2.6 vs. 5.9 ±2.8), and ODI (22.4% ± 18.6 vs. 45.3% ± 15.3), as well as health-related quality of life (EQ-5D index: 0.71 ±0.28 vs. 0.34 ±0.32). More of the professional workers were working at one year than those prior to surgery (70.3% vs. 55.2%). Three AEs and one serious AE were considered procedure-related; there were no deep site infections or deaths. This is the first study evaluating MILIF for treatment of DLD in daily clinical practice. Clinically significant improvements were observed in all endpoints. Short-term post-surgery improvements (four weeks) were maintained through one year with minimal complications. Our results suggest that MILIF has good-to-excellent outcomes for the treatment of DLD in a broad patient population under different clinical conditions and healthcare delivery systems.
Keywords: degenerative lumbar disorders; minimal access spinal technologies; minimally invasive lumbar fusion; patient-reported outcomes; pragmatic.
Conflict of interest statement
The authors have declared financial relationships, which are detailed in the next section.
Figures
References
-
- Minimally invasive fusion: summary statement. Guyer RD, Foley KT, Phillips FM, Ball PA. Spine. 2003;28:0. - PubMed
-
- Minimally invasive spine surgery. McAfee PC, Phillips FM, Andersson G, et al. Spine. 2010;35:0. - PubMed
-
- Minimally invasive transforaminal lumbar interbody fusion: a review of techniques and outcomes. Karikari IO, Isaacs RE. Spine. 2010;35:0. - PubMed
-
- Minimally invasive transforaminal lumbar interbody fusion for degenerative spine. Chaudhary KS, Groff MW. Tech Orthop. 2011;26:146–155.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous