

A Systematic Review of Clinical Outcomes and Prognostic Factors for Patients Undergoing Surgery for Spinal Metastases Secondary to Breast Cancer
- PMID: 27433433
- PMCID: PMC4947406
- DOI: 10.1055/s-0035-1564807
A Systematic Review of Clinical Outcomes and Prognostic Factors for Patients Undergoing Surgery for Spinal Metastases Secondary to Breast Cancer
Abstract
Study design: Review of the literature.
Objective: Surgery and cement augmentation procedures are effective palliative treatment of symptomatic spinal metastases. Our objective is to systematically review the literature to describe the survival, prognostic factors, and clinical outcomes of surgery and cement augmentation procedures for breast cancer metastases to the spine.
Methods: We performed a literature review using PubMed to identify articles that reported outcomes and/or prognostic factors of the breast cancer patient population with spinal metastases treated with any surgical technique since 1990.
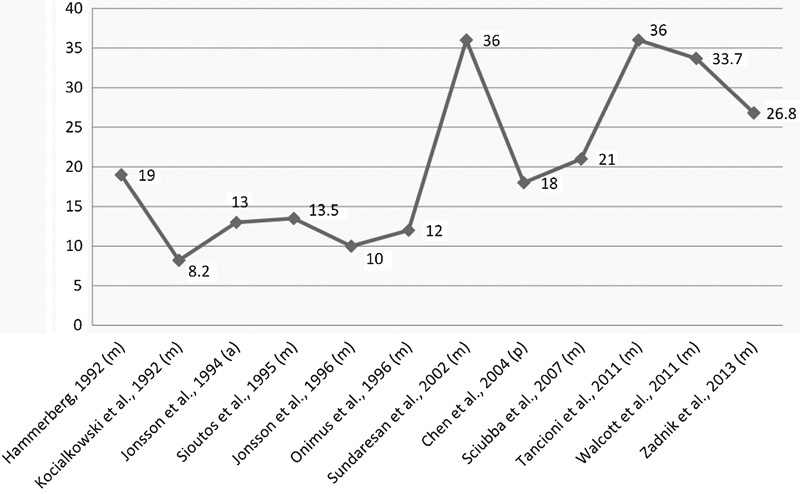
Results: The median postoperative survival for metastatic breast cancer was 21.7 months (8.2 to 36 months), the mean rate of any pain improvement was 92.9% (76 to 100%), the mean rate of neurologic improvement was 63.8% (53 to 100%), the mean rate of neurologic decline was 4.1% (0 to 8%), and the local tumor control rate was 92.6% (89 to 100%). Kyphoplasty studies reported a high rate of pain control in selected patients. Negative prognostic variables included hormonal (estrogen and progesterone) and human epidermal growth factor receptor 2 (HER2) receptor refractory tumor status, high degree of axillary lymph node involvement, and short disease-free interval (DFI). All other clinical or prognostic parameters were of low or insufficient strength.
Conclusion: With respect to clinical outcomes, surgery consistently yielded neurologic improvements in patients presenting with a deficit with a minimal risk of worsening; however, negative prognostic factors associated with shorter survival following surgery include estrogen receptor/progesterone receptor negativity, HER2 negativity, and a short DFI.
Keywords: breast cancer; kyphoplasty; metastasis; spine; surgery; survival; tumor; vertebroplasty.
Conflict of interest statement
Figures
Similar articles
-
Neurologic, functional, and survival outcomes following surgical management of metastatic breast cancer to the spine.Clin Neurol Neurosurg. 2022 Sep;220:107360. doi: 10.1016/j.clineuro.2022.107360. Epub 2022 Jul 5. Clin Neurol Neurosurg. 2022. PMID: 35868202
-
Prognostic factors in patients with spinal metastasis: a systematic review and meta-analysis.Spine J. 2017 May;17(5):689-708. doi: 10.1016/j.spinee.2016.12.003. Epub 2016 Dec 14. Spine J. 2017. PMID: 27988342
-
[Clinicopathological features and prognostic factors of breast cancer patients with inguinal lymph node metastases: a report of 17 cases].Zhonghua Zhong Liu Za Zhi. 2013 Mar;35(3):207-11. doi: 10.3760/cma.j.issn.0253-3766.2013.03.010. Zhonghua Zhong Liu Za Zhi. 2013. PMID: 23880002 Chinese.
-
Overview of resistance to systemic therapy in patients with breast cancer.Adv Exp Med Biol. 2007;608:1-22. doi: 10.1007/978-0-387-74039-3_1. Adv Exp Med Biol. 2007. PMID: 17993229 Review.
-
Percutaneous vertebroplasty for patients with metastatic compression fractures of the thoracolumbar spine: clinical and radiological factors affecting functional outcomes.Spine J. 2016 Mar;16(3):355-64. doi: 10.1016/j.spinee.2015.11.033. Epub 2015 Dec 2. Spine J. 2016. PMID: 26656435
Cited by
-
Practice variations in indication, timing and outcome of Multiple Myeloma patients undergoing surgery for vertebral lesions - results from the European M2Spine study group.J Neurooncol. 2025 Sep;174(3):765-777. doi: 10.1007/s11060-025-05085-y. Epub 2025 Jun 13. J Neurooncol. 2025. PMID: 40512280 Free PMC article.
-
Anti-Tumor Effects of Low Dose Zoledronate on Lung Cancer-Induced Spine Metastasis.J Clin Med. 2019 Aug 14;8(8):1212. doi: 10.3390/jcm8081212. J Clin Med. 2019. PMID: 31416169 Free PMC article.
-
Natural History and Prognostic Factors of Cholangiocarcinoma With Spinal Metastasis: A 10-Year Single Center Study.Clin Spine Surg. 2018 Apr;31(3):E160-E165. doi: 10.1097/BSD.0000000000000625. Clin Spine Surg. 2018. PMID: 29596214 Free PMC article.
-
Survival Trends After Surgery for Spinal Metastatic Tumors: 20-Year Cancer Center Experience.Neurosurgery. 2021 Jan 13;88(2):402-412. doi: 10.1093/neuros/nyaa380. Neurosurgery. 2021. PMID: 32970144 Free PMC article.
-
Aldehyde dehydrogenase 1 (ALDH1) immunostaining in axillary lymph node metastases is an independent prognostic factor in ALDH1-positive breast cancer.J Int Med Res. 2021 Oct;49(10):3000605211047279. doi: 10.1177/03000605211047279. J Int Med Res. 2021. PMID: 34644211 Free PMC article.
References
-
- Esteva F J, Valero V, Pusztai L, Boehnke-Michaud L, Buzdar A U, Hortobagyi G N. Chemotherapy of metastatic breast cancer: what to expect in 2001 and beyond. Oncologist. 2001;6(2):133–146. - PubMed
-
- American Cancer Society . Atlanta, GA: American Cancer Society; 2014. Cancer Facts & Figures 2014.
-
- Zadnik P L, Hwang L, Ju D G. et al.Prolonged survival following aggressive treatment for metastatic breast cancer in the spine. Clin Exp Metastasis. 2014;31(1):47–55. - PubMed
-
- Eleraky M, Papanastassiou I, Vrionis F D. Management of metastatic spine disease. Curr Opin Support Palliat Care. 2010;4(3):182–188. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
