

Minimally Invasive Transforaminal Lumbar Interbody Fusion at L5-S1 through a Unilateral Approach: Technical Feasibility and Outcomes
- PMID: 27433472
- PMCID: PMC4940521
- DOI: 10.1155/2016/2518394
Minimally Invasive Transforaminal Lumbar Interbody Fusion at L5-S1 through a Unilateral Approach: Technical Feasibility and Outcomes
Abstract
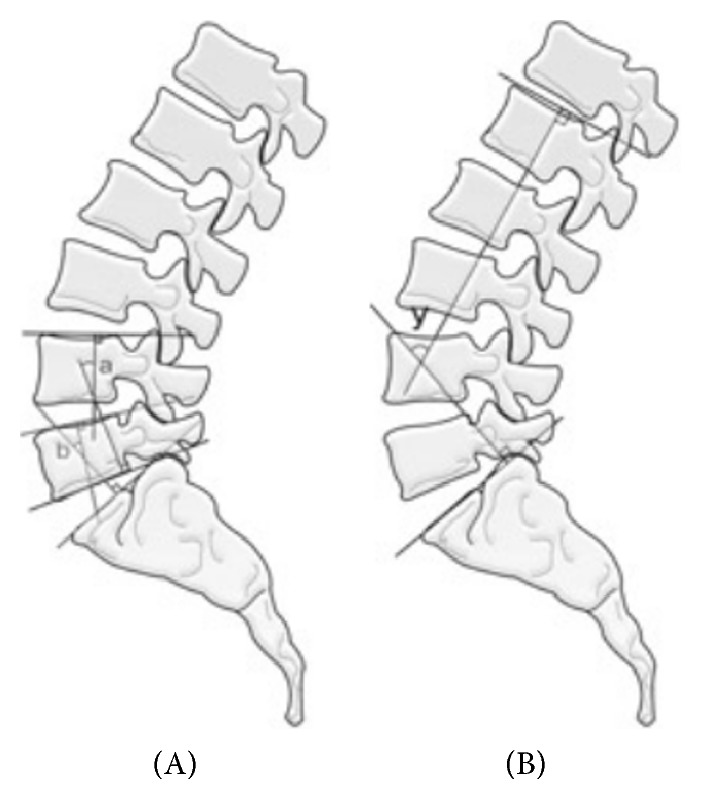
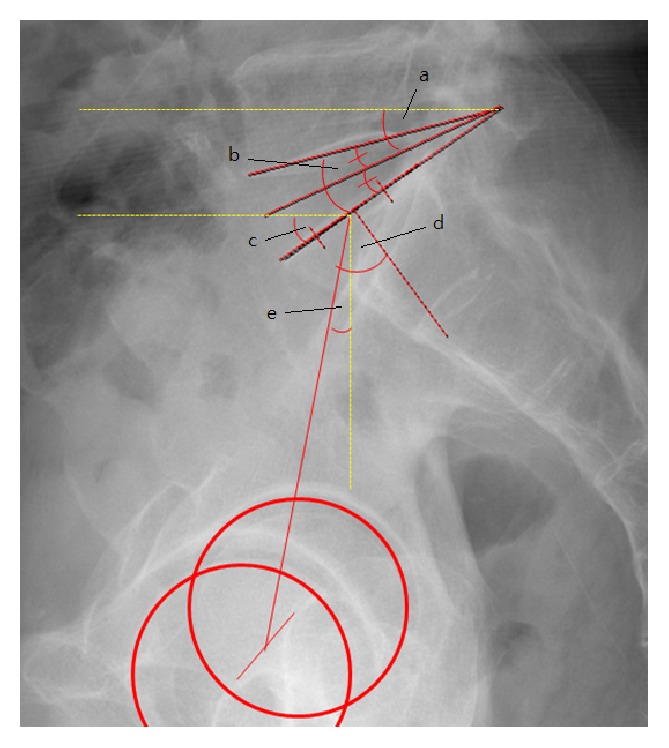
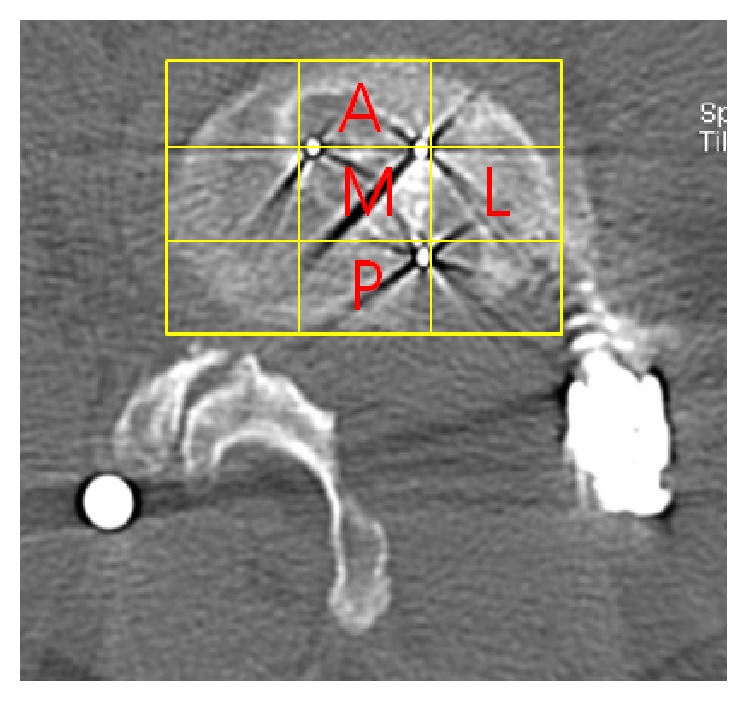
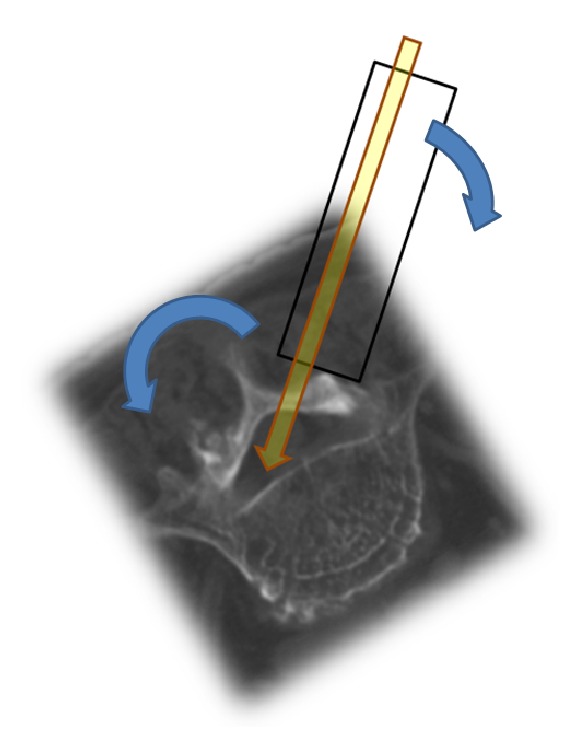
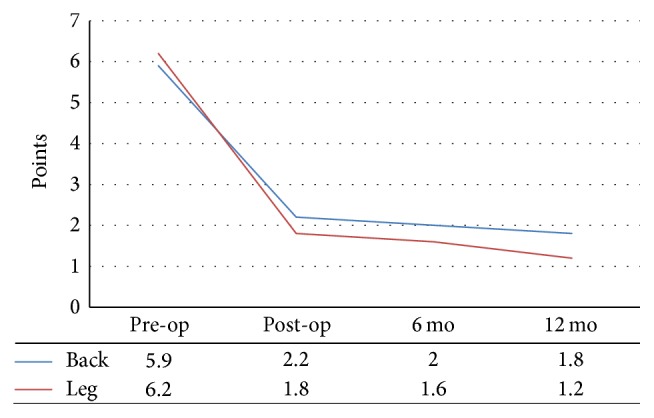
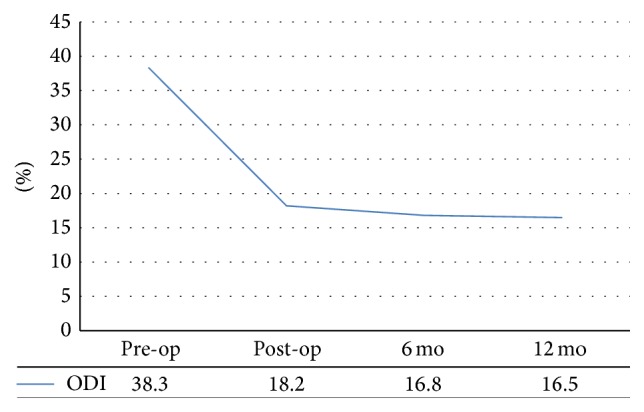
Background. Minimally invasive spinal transforaminal lumbar interbody fusion (MIS-TLIF) at L5-S1 is technically more demanding than it is at other levels because of the anatomical and biomechanical traits. Objective. To determine the clinical and radiological outcomes of MIS-TLIF for treatment of single-level spinal stenosis low-grade isthmic or degenerative spondylolisthesis at L5-S1. Methods. Radiological data and electronic medical records of patients who underwent MIS-TLIF between May 2012 and December 2014 were reviewed. Fusion rate, cage position, disc height (DH), disc angle (DA), disc slope angle, segmental lordotic angle (SLA), lumbar lordotic angle (LLA), and pelvic parameters were assessed. For functional assessment, the visual analogue scale (VAS), Oswestry disability index (ODI), and patient satisfaction rate (PSR) were utilized. Results. A total of 21 levels in 21 patients were studied. DH, DA, SLA, and LLA had increased from their preoperative measures at the final follow-up. Fusion rate was 86.7% (18/21) at 12 months' follow-up. The most common cage position was anteromedial (15/21). The mean VAS scores for back and leg pain mean ODI scores improved significantly at the final follow-up. PSR was 88%. Cage subsidence was observed in 33.3% (7/21). Conclusions. The clinical and radiologic outcomes after MIS-TLIF at L5-S1 in patients with spinal stenosis or spondylolisthesis are generally favorable.
Figures
References
-
- Sheehan J. M., Shaffrey C. I., Jane J. A., Sr. Degenerative lumbar stenosis: the neurosurgical perspective. Clinical Orthopaedics and Related Research. 2001;(384):61–74. - PubMed
-
- Foley K. T., Holly L. T., Schwender J. D. Minimally invasive lumbar fusion. Spine. 2003;28(15):S26–S35. - PubMed
-
- Holly L. T., Schwender J. D., Rouben D. P., Foley K. T. Minimally invasive transforaminal lumbar interbody fusion: indications, technique, and complications. Neurosurgical Focus. 2006;20(3):p. E6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
