

Liver Resection and Transplantation for Patients With Hepatocellular Carcinoma Beyond Milan Criteria
- PMID: 27433910
- PMCID: PMC5279918
- DOI: 10.1097/SLA.0000000000001866
Liver Resection and Transplantation for Patients With Hepatocellular Carcinoma Beyond Milan Criteria
Abstract
Objectives: To assess survival after liver resection and transplantation in patients with hepatocellular carcinoma (HCC) beyond Milan criteria.
Background: The role of liver resection and transplantation remains controversial for patients with HCC beyond Milan criteria. Resection of advanced tumors and transplantation using extended-criteria are pursued at select high-volume center.
Methods: Patients from 5 liver cancer centers in the United States who had liver resection or transplantation for HCC beyond Milan criteria between 1990 and 2011 were included in the study. Multivariable and propensity-matching analyses estimated the effects of clinical factors and operative selection on survival.
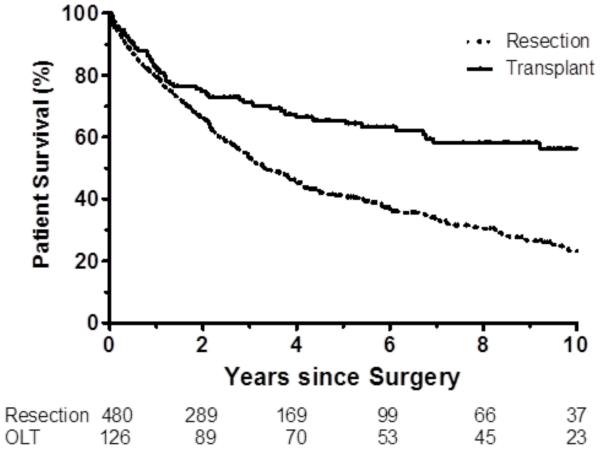
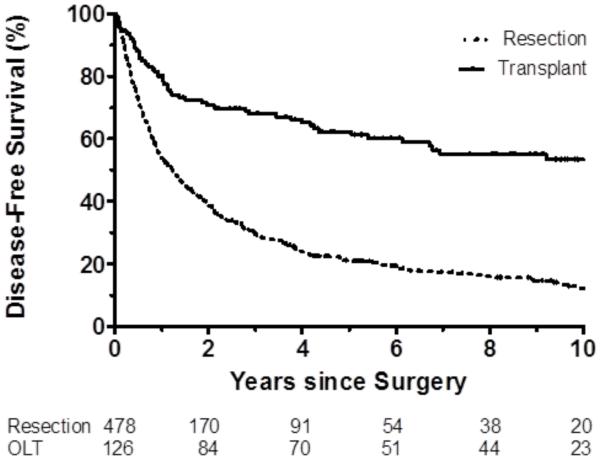
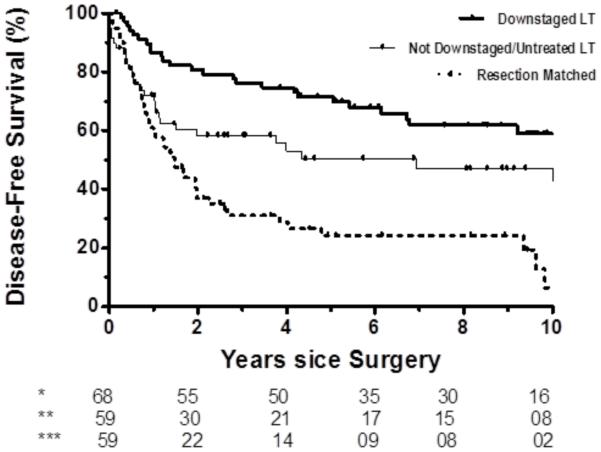
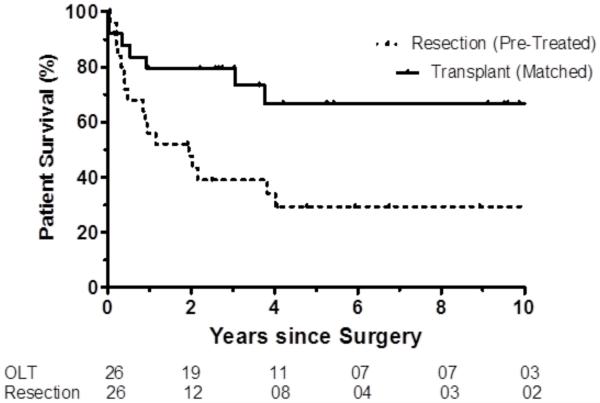
Results: Of 608 patients beyond Milan without vascular invasion, 480 (79%) patients underwent resection and 128 (21%) underwent transplantation. Clinicopathologic profiles between resection and transplant patients differed significantly. Hepatitis C and cirrhosis were more prevalent in transplantation group (P < 0.001). Resection patients had larger tumors [median 9 cm, interquartile range (IQR): 6.5-12.9 cm vs. median 4.1, IQR: 3.4-5.3 cm, P < 0.001]; transplant patients were more likely to have multiple tumors (78% vs 28%, P < 0.001).Overall (OS) and disease-free survival (DFS) were both greater after tumor downstaging and transplantation than resection (all P < 0.001). OS did not differ between liver transplant recipients who were not pretreated or pretreated and failed to downstage compared with propensity-matched liver resection patients (P ≥ 0.176); DFS in this propensity matched cohort was greater after liver transplantation (P ≤ 0.017).
Conclusions: Liver resection and transplantation provide curative options for patients with HCC beyond Milan criteria. Further treatment strategies aimed at the efficiency and durability of tumor downstaging and expansion of the role of transplantation among suitable candidates could improve outcomes in patients with large or multifocal HCC.
Figures




Comment in
-
Resection versus transplantation for hepatocellular carcinoma exceeding Milan criteria within increasing donor shortage.Hepatobiliary Surg Nutr. 2017 Aug;6(4):280-283. doi: 10.21037/hbsn.2017.03.14. Hepatobiliary Surg Nutr. 2017. PMID: 28848755 Free PMC article. No abstract available.
-
Resection or transplantation for hepatocellular carcinoma: is the decision clear for patients beyond Milan criteria?Hepatobiliary Surg Nutr. 2017 Aug;6(4):284-286. doi: 10.21037/hbsn.2017.04.03. Hepatobiliary Surg Nutr. 2017. PMID: 28848756 Free PMC article. No abstract available.
-
Appropriate surgical therapy for patients with hepatocellular carcinoma beyond Milan criteria.Hepatobiliary Surg Nutr. 2017 Oct;6(5):327-328. doi: 10.21037/hbsn.2017.05.06. Hepatobiliary Surg Nutr. 2017. PMID: 29152479 Free PMC article. No abstract available.
References
-
- Forner A, Gilabert M, Bruix J, et al. Treatment of intermediate-stage hepatocellular carcinoma. Nat Rev Clin Oncol. 2014;11:525–535. - PubMed
-
- Guy J, Kelley RK, Roberts J, et al. Multidisciplinary management of hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2012;10:354–362. - PubMed
-
- Torzilli G, Belghiti J, Kokudo N, et al. A snapshot of the effective indications and results of surgery for hepatocellular carcinoma in tertiary referral centers: is it adherent to the EASL/AASLD recommendations?: an observational study of the HCC East-West study group. Ann Surg. 2013;257:929–937. - PubMed
-
- Yao FY, Xiao L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: validation of the UCSF-expanded criteria based on preoperative imaging. Am J Transplant. 2007;7:2587–2596. - PubMed
-
- Onaca N, Davis GL, Goldstein RM, et al. Expanded criteria for liver transplantation in patients with hepatocellular carcinoma: a report from the International Registry of Hepatic Tumors in Liver Transplantation. Liver Transpl. 2007;13:391–399. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
