

Treatments for the prevention of Sudden Unexpected Death in Epilepsy (SUDEP)
- PMID: 27434597
- PMCID: PMC6458047
- DOI: 10.1002/14651858.CD011792.pub2
Treatments for the prevention of Sudden Unexpected Death in Epilepsy (SUDEP)
Update in
-
Treatments for the prevention of Sudden Unexpected Death in Epilepsy (SUDEP).Cochrane Database Syst Rev. 2020 Apr 2;4(4):CD011792. doi: 10.1002/14651858.CD011792.pub3. Cochrane Database Syst Rev. 2020. PMID: 32239759 Free PMC article.
Abstract
Background: Sudden Unexpected Death in Epilepsy (SUDEP) is defined as sudden, unexpected, witnessed or unwitnessed, non-traumatic or non-drowning death of people with epilepsy, with or without evidence of a seizure, excluding documented status epilepticus and in whom postmortem examination does not reveal a structural or toxicological cause for death. SUDEP has a reported incidence of 1 to 2 per 1000 patient years and represents the most common epilepsy-related cause of death. The presence and frequency of generalised tonic-clonic seizures (GTCS), male sex, early age of seizure onset, duration of epilepsy, and polytherapy are all predictors of risk of SUDEP. The exact pathophysiology of SUDEP is currently unknown, although GTCS-induced cardiac, respiratory, and brainstem dysfunction appears likely. Appropriately chosen antiepileptic drug treatment can render around 70% of patients free of all seizures. However, around one-third will remain drug refractory despite polytherapy. Continuing seizures place patients at risk of SUDEP, depression, and reduced quality of life. Preventative strategies for SUDEP include reducing the occurrence of GTCS by timely referral for presurgical evaluation in people with lesional epilepsy and advice on lifestyle measures; detecting cardiorespiratory distress through clinical observation and seizure, respiratory, and heart rate monitoring devices; preventing airway obstruction through nocturnal supervision and safety pillows; reducing central hypoventilation through physical stimulation and enhancing serotonergic mechanisms of respiratory regulation using selective serotonin reuptake inhibitors (SSRIs); reducing adenosine and endogenous opioid-induced brain and brainstem depression.
Objectives: To assess the effectiveness of interventions in preventing SUDEP in people with epilepsy by synthesising evidence from randomised controlled trials of interventions and cohort and case-control non-randomised studies.
Search methods: We searched the following databases: Cochrane Epilepsy Group Specialized Register; Cochrane Central Register of Controlled Trials (CENTRAL, Issue 11, 2015) via the Cochrane Register of Studies Online (CRSO); MEDLINE (Ovid, 1946 onwards); SCOPUS (1823 onwards); PsycINFO (EBSCOhost, 1887 onwards); CINAHL Plus (EBSCOhost, 1937 onwards); ClinicalTrials.gov; and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP). We used no language restrictions. The date of the last search was 12 November 2015. We checked the reference lists of retrieved studies for additional reports of relevant studies and contacted lead study authors for any relevant unpublished material. We identified duplicate studies by screening reports according to title, authors' names, location, and medical institute, omitting any duplicated studies. We identified any grey literature studies published in the last five years by searching: Zetoc database; ISI Proceedings; International Bureau for Epilepsy (IBE) congress proceedings database; International League Against Epilepsy (ILAE) congress proceedings database; abstract books of symposia and congresses, meeting abstracts, and research reports.
Selection criteria: We aimed to include randomised controlled trials (RCTs), quasi-RCTs, and cluster-RCTs; prospective non-randomised cohort controlled and uncontrolled studies; and case-control studies of adults and children with epilepsy receiving an intervention for the prevention of SUDEP. Types of interventions included: early versus delayed pre-surgical evaluation for lesional epilepsy; educational programmes; seizure-monitoring devices; safety pillows; nocturnal supervision; selective serotonin reuptake inhibitors (SSRIs); opiate antagonists; and adenosine antagonists.
Data collection and analysis: We aimed to collect data on study design factors and participant demographics for included studies. The primary outcome of interest was the number of deaths from SUDEP. Secondary outcomes included: number of other deaths (unrelated to SUDEP); change in mean depression and anxiety scores (as defined within the study); clinically important change in quality of life, that is any change in quality of life score (average and endpoint) according to validated quality of life scales; and number of hospital attendances for seizures.
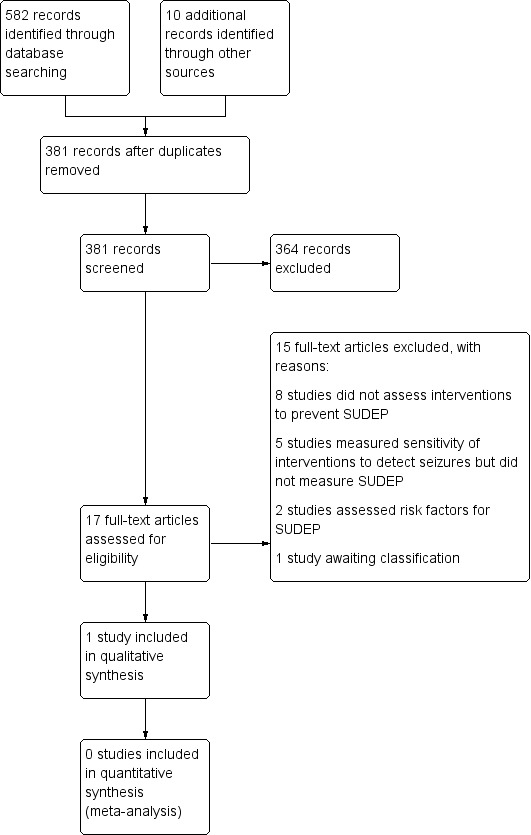
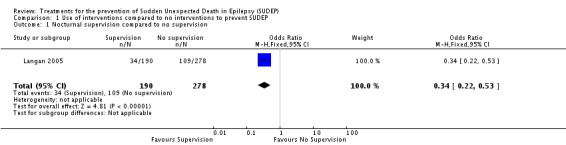
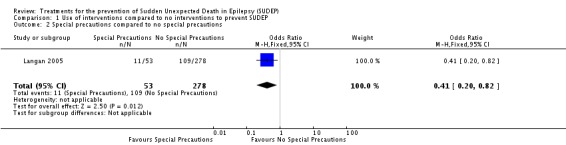
Main results: We identified 582 records from the databases and search strategies. We found 10 further records by searching other resources (handsearching). We removed 211 duplicate records and screened 381 records (title and abstract) for inclusion in the review. We excluded 364 records based on the title and abstract and assessed 17 full-text articles. We excluded 15 studies: eight studies did not assess interventions to prevent SUDEP; five studies measured sensitivity of devices to detect GTCS but did not directly measure SUDEP; and two studies assessed risk factors for SUDEP but not interventions for preventing SUDEP. One listed study is awaiting classification.We included one case-control study at serious risk of bias within a qualitative analysis in this review. This study of 154 cases of SUDEP and 616 controls ascertained a protective effect for the presence of nocturnal supervision (unadjusted odds ratio (OR) 0.34, 95% confidence interval (CI) 0.22 to 0.53) and when a supervising person shared the same bedroom or when special precautions, for example a listening device, were used (unadjusted OR 0.41, 95% CI 0.20 to 0.82). This effect was independent of seizure control. Non-SUDEP deaths; changes to anxiety, depression, and quality of life; and number of hospital attendances were not reported.
Authors' conclusions: We found very low-quality evidence of a preventative effect for nocturnal supervision against SUDEP. Further research is required to identify the effectiveness of other current interventions, for example seizure detection devices, safety pillows, SSRIs, early surgical evaluation, educational programmes, and opiate and adenosine antagonists in preventing SUDEP in people with epilepsy.
Conflict of interest statement
Melissa J Maguire: none known.
Cerian F Jackson: none known.
Anthony G Marson: A consortium of pharmaceutical companies (GSK, EISAI, UCB Pharma) funded the National Audit of Seizure Management in Hospitals (NASH) through grants paid to University of Liverpool. Professor Tony Marson is Theme Leader for Managing Complex Needs at NIHR CLAHRC NWC.
Sarah J Nolan: none known.
Figures
Similar articles
-
Treatments for the prevention of Sudden Unexpected Death in Epilepsy (SUDEP).Cochrane Database Syst Rev. 2020 Apr 2;4(4):CD011792. doi: 10.1002/14651858.CD011792.pub3. Cochrane Database Syst Rev. 2020. PMID: 32239759 Free PMC article.
-
Treatments for seizures in catamenial (menstrual-related) epilepsy.Cochrane Database Syst Rev. 2021 Sep 16;9(9):CD013225. doi: 10.1002/14651858.CD013225.pub3. Cochrane Database Syst Rev. 2021. PMID: 34528245 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Prognosis of adults and children following a first unprovoked seizure.Cochrane Database Syst Rev. 2023 Jan 23;1(1):CD013847. doi: 10.1002/14651858.CD013847.pub2. Cochrane Database Syst Rev. 2023. PMID: 36688481 Free PMC article.
-
Carbamazepine versus phenobarbitone monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2016 Dec 15;12(12):CD001904. doi: 10.1002/14651858.CD001904.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2018 Oct 24;10:CD001904. doi: 10.1002/14651858.CD001904.pub4. PMID: 27976799 Free PMC article. Updated.
Cited by
-
The hidden rhythms of epilepsy: exploring biological clocks and epileptic seizure dynamics.Acta Epileptol. 2025 Jan 3;7(1):1. doi: 10.1186/s42494-024-00197-w. Acta Epileptol. 2025. PMID: 40217344 Free PMC article. Review.
-
Experimental Therapeutic Strategies in Epilepsies Using Anti-Seizure Medications.J Exp Pharmacol. 2021 Mar 11;13:265-290. doi: 10.2147/JEP.S267029. eCollection 2021. J Exp Pharmacol. 2021. PMID: 33732031 Free PMC article. Review.
-
Let's talk SUDEP.Noro Psikiyatr Ars. 2019 Sep 5;56(4):292-301. doi: 10.29399/npa.23663. eCollection 2019 Dec. Noro Psikiyatr Ars. 2019. PMID: 31903040 Free PMC article. Review.
-
Socioeconomic inequalities in hospitalizations for chronic ambulatory care sensitive conditions: a systematic review of peer-reviewed literature, 1990-2018.Int J Equity Health. 2020 May 4;19(1):60. doi: 10.1186/s12939-020-01160-0. Int J Equity Health. 2020. PMID: 32366253 Free PMC article.
-
Has the Time Come to Stratify and Score SUDEP Risk to Inform People With Epilepsy of Their Changes in Safety?Front Neurol. 2018 Apr 27;9:281. doi: 10.3389/fneur.2018.00281. eCollection 2018. Front Neurol. 2018. PMID: 29755403 Free PMC article.
References
References to studies included in this review
-
- Langan Y, Nashef L, Sander JW. Case‐control study of SUDEP. Neurology 2005;64(7):1131‐3. - PubMed
References to studies excluded from this review
-
- Almeida AG, Nunes ML, Palmini ALF, Costa JC. Incidence of SUDEP in a cohort of patients with refractory epilepsy: the role of surgery and lesion localization. Arquivos de Neuro‐Psiquiatria 2010;68(6):898‐902. - PubMed
-
- Annegers JF, Coan SP, Hauser WA, Leestma J, Duffell W, Tarver B. Epilepsy, vagal nerve stimulation by the NCP system, mortality, and sudden, unexpected, unexplained death. Epilepsia 1998;39(2):206‐12. - PubMed
-
- Annegers JF, Coan SP, Hauser WA, Leestma J. Epilepsy, vagal nerve stimulation by the NCP system, all‐cause mortality, and sudden, unexpected, unexplained death. Epilepsia 2000;41(5):549‐53. - PubMed
-
- Bateman LM, Li CS, Lin TC, Seyal M. Serotonin reuptake inhibitors are associated with reduced severity of ictal hypoxemia in medically refractory partial epilepsy. Epilepsia 2010;51(10):2211‐4. - PubMed
-
- Beniczky S, Polster T, Kjaer TW, Hjalgrim H. Detection of generalized tonic‐clonic seizures by a wireless wrist accelerometer: a prospective, multicenter study. Epilepsia 2013;54(4):e58‐61. - PubMed
References to studies awaiting assessment
-
- NCT00736424. Brain stimulation for epilepsy long term follow‐up (SUDEP). http://clinicaltrials.gov/show/NCT00736424.
Additional references
-
- Sterne JAC, Higgins JPT, Reeves BC on behalf of the development group for ACROBAT‐NRSI. A Cochrane Risk Of Bias Assessment Tool: for Non‐Randomized Studies of Interventions (ACROBAT‐NRSI), Version 1.0.0, 24 September 2014. Available from http://www.riskofbias.info (accessed 5 January 2015).
-
- Dasheiff RM. Sudden unexpected death in epilepsy: a series from an epilepsy surgery program and speculation on the relationship to sudden cardiac death. Journal of Clinical Neurophysiology 1991;8(2):216‐22. - PubMed
-
- Devinsky O. Sudden, unexpected death in epilepsy. The New England Journal of Medicine 2012;365(19):1801‐11. - PubMed
-
- Favale E, Rubino V, Mainardi P, Lunardi G, Albano C. Anticonvulsant effect of fluoxetine in humans. Neurology 1995;45(10):1926‐7. - PubMed
-
- Favale E, Audenino D, Cocito L, Albano C. The anticonvulsant effect of citalopram as an indirect evidence of serotonergic impairment in human epileptogenesis. Seizure 2003;12(5):316‐8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical