

Preterm neonatal urinary renal developmental and acute kidney injury metabolomic profiling: an exploratory study
- PMID: 27435284
- PMCID: PMC5123933
- DOI: 10.1007/s00467-016-3439-9
Preterm neonatal urinary renal developmental and acute kidney injury metabolomic profiling: an exploratory study
Abstract
Background: Acute kidney injury (AKI) staging has been developed in the adult and pediatric populations, but these do not yet exist for the neonatal population. Metabolomics was utilized to uncover biomarkers of normal and AKI-associated renal function in preterm infants. The study comprised 20 preterm infants with an AKI diagnosis who were matched by gestational age and gender to 20 infants without an AKI diagnosis.
Methods: Urine samples from pre-term newborn infants collected on day 2 of life were analyzed using broad-spectrum nuclear magnetic resonance (NMR) metabolomics. Multivariate analysis methods were used to identify metabolite profiles that differentiated AKI and no AKI, and to identify a metabolomics profile correlating with gestational age in infants with and without AKI.
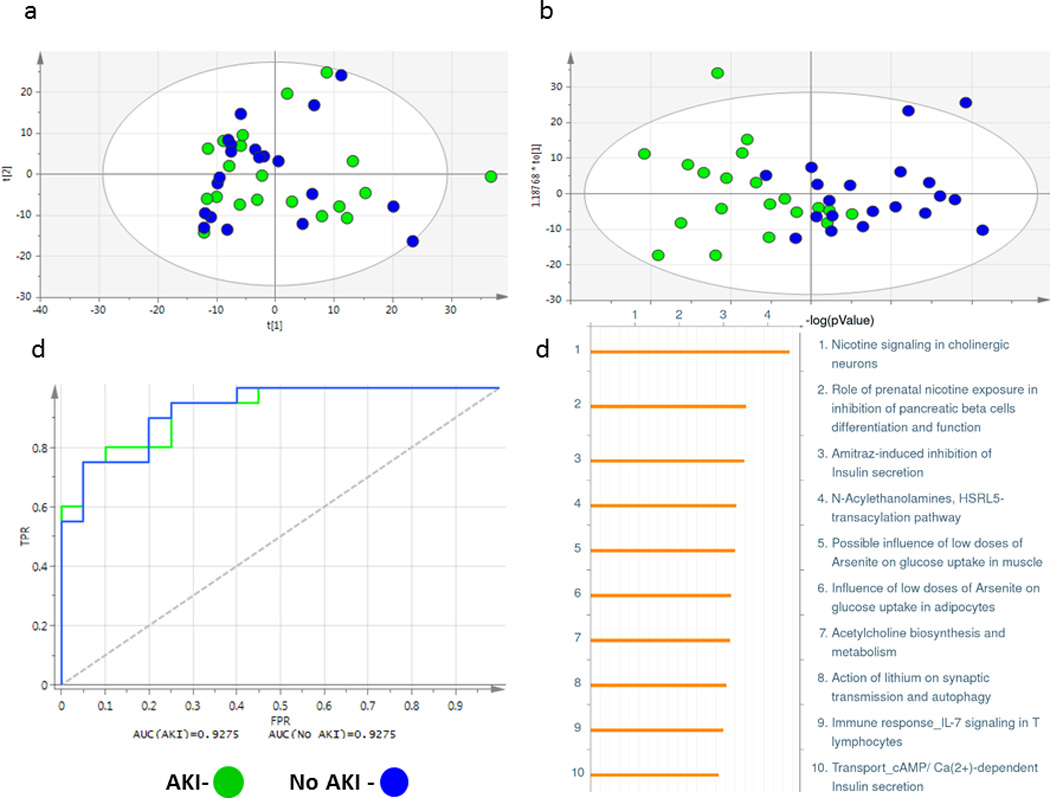
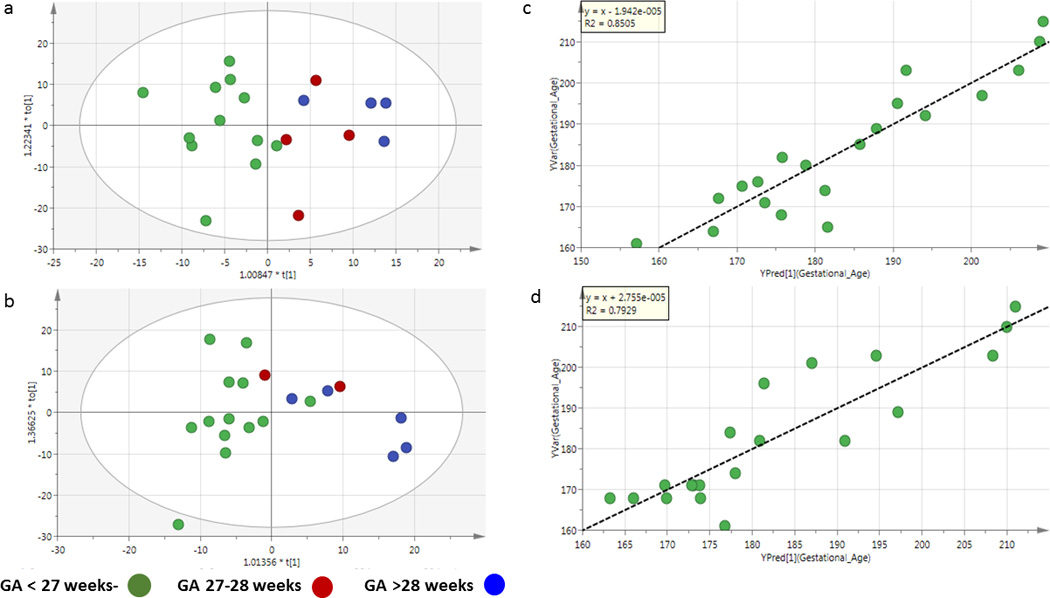
Results: There was a clear distinction between the AKI and no-AKI profiles. Two previously identified biomarkers of AKI, hippurate and homovanillate, differentiated AKI from no-AKI profiles. Pathway analysis revealed similarities to cholinergic neurons, prenatal nicotine exposure on pancreatic β cells, and amitraz-induced inhibition of insulin secretion. Additionally, a pH difference was noted. Both pH and the metabolites were found to be associated with AKI; however, only the metabotype was a significant predictor of AKI. Pathways for the no-AKI group that correlated uniquely with gestational age included aminoacyl-t-RNA biosynthesis, whereas pathways in the AKI group yielded potential metabolite changes in pyruvate metabolism.
Conclusions: Metabolomics was able to differentiate the urinary profiles of neonates with and without an AKI diagnosis and metabolic developmental profiles correlated with gestational age. Further studies in larger cohorts are needed to validate these results.
Keywords: Acute kidney injury; Metabolomics; Multivariate analysis; NMR spectroscopy; Neonatal; Regression analysis; Renal development.
Figures



References
-
- Askenazi DJ, Feig DI, Graham NM, Hui-Stickle S, Goldstein SL. 3–5 year longitudinal follow-up of pediatric patients after acute renal failure. Kidney international. 2006;69:184–189. - PubMed
-
- Viswanathan S, Manyam B, Azhibekov T, Mhanna MJ. Risk factors associated with acute kidney injury in extremely low birth weight (ELBW) infants. Pediatric nephrology (Berlin, Germany) 2012;27:303–311. - PubMed
-
- Koralkar R, Ambalavanan N, Levitan EB, McGwin G, Goldstein S, Askenazi D. Acute kidney injury reduces survival in very low birth weight infants. Pediatric research. 2011;69:354–358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
