

Can genetic evidence help us to understand the fetal origins of type 2 diabetes?
- PMID: 27435863
- PMCID: PMC4973887
- DOI: 10.1007/s00125-016-4057-6
Can genetic evidence help us to understand the fetal origins of type 2 diabetes?
Abstract
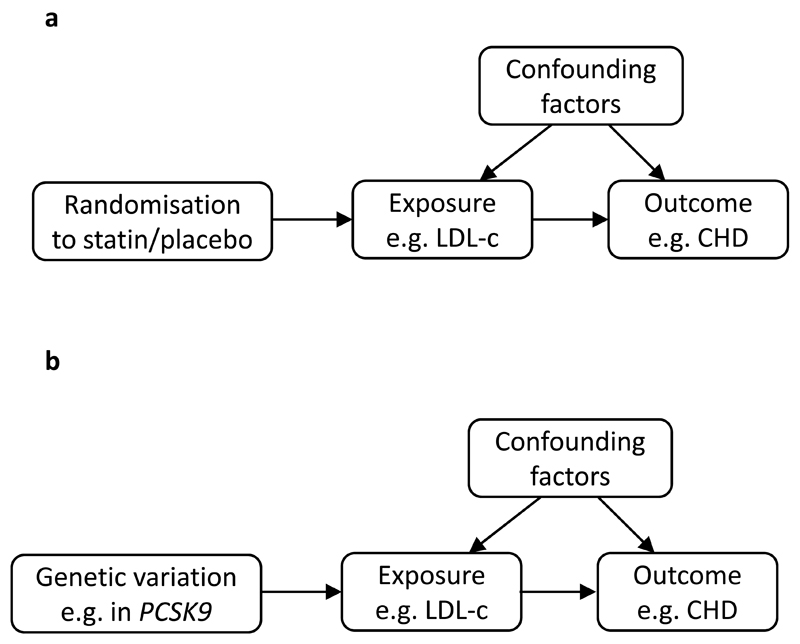
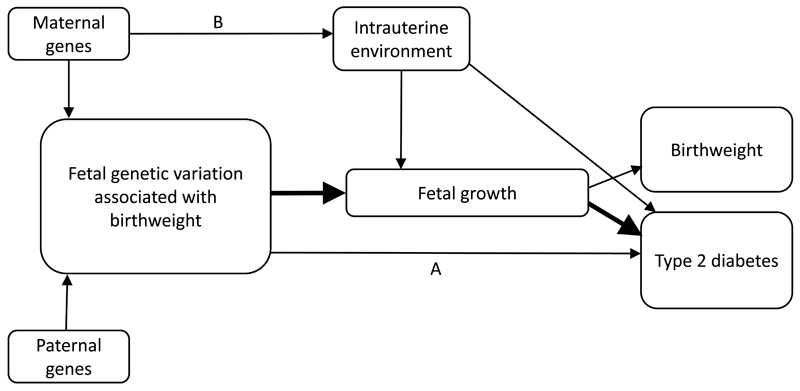
Lower birthweight is consistently associated with a higher risk of type 2 diabetes in observational studies, but the mechanisms underlying this association are not fully understood. Animal models and studies of famine-exposed populations have provided support for the developmental origins hypothesis, under which exposure to poor intrauterine nutrition results in reduced fetal growth and also contributes to the developmental programming of later type 2 diabetes risk. However, testing this hypothesis is difficult in human studies and studies aiming to do so are mostly observational and have limited scope for causal inference due to the presence of confounding factors. In this issue of Diabetologia, Wang et al (doi: 10.1007/s00125-016-4019-z ) have used genetic variation associated with birthweight in a Mendelian randomisation analysis to assess evidence of a causal link between fetal growth and type 2 diabetes. Mendelian randomisation offers the potential to examine associations between exposures and outcomes in the absence of factors that would normally confound observational studies. This commentary discusses the results of the Mendelian randomisation study carried out by Wang et al, in relation to the study design and its limitations. Challenges and opportunities for future studies are also outlined.
Keywords: Birthweight; Fetal growth; Genetics; Genome-wide association study; Instrumental variable; Mendelian randomisation; Pleiotropy; Type 2 diabetes.
Conflict of interest statement
The author declares that there is no duality of interest associated with this manuscript.
Figures
Comment on
-
Low birthweight and risk of type 2 diabetes: a Mendelian randomisation study.Diabetologia. 2016 Sep;59(9):1920-7. doi: 10.1007/s00125-016-4019-z. Epub 2016 Jun 23. Diabetologia. 2016. PMID: 27333884 Free PMC article.
References
-
- Harder T, Rodekamp E, Schellong K, Dudenhausen JW, Plagemann A. Birth weight and subsequent risk of type 2 diabetes: a meta-analysis. Am J Epidemiol. 2007;165:849–857. - PubMed
-
- de Rooij SR, Painter RC, Roseboom TJ, et al. Glucose tolerance at age 58 and the decline of glucose tolerance in comparison with age 50 in people prenatally exposed to the Dutch famine. Diabetologia. 2006;49:637–643. - PubMed
-
- Poulsen P, Vaag AA, Kyvik KO, Moller Jensen D, Beck-Nielsen H. Low birth weight is associated with NIDDM in discordant monozygotic and dizygotic twin pairs. Diabetologia. 1997;40:439–446. - PubMed
-
- Warner MJ, Ozanne SE. Mechanisms involved in the developmental programming of adulthood disease. Biochem J. 2010;427:333–347. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
