

Postmortem genetic screening for the identification, verification, and reporting of genetic variants contributing to the sudden death of the young
- PMID: 27435932
- PMCID: PMC5052040
- DOI: 10.1101/gr.195800.115
Postmortem genetic screening for the identification, verification, and reporting of genetic variants contributing to the sudden death of the young
Abstract
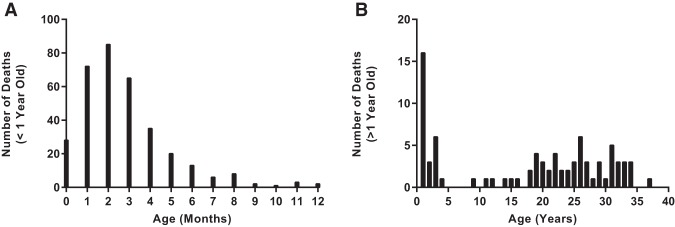
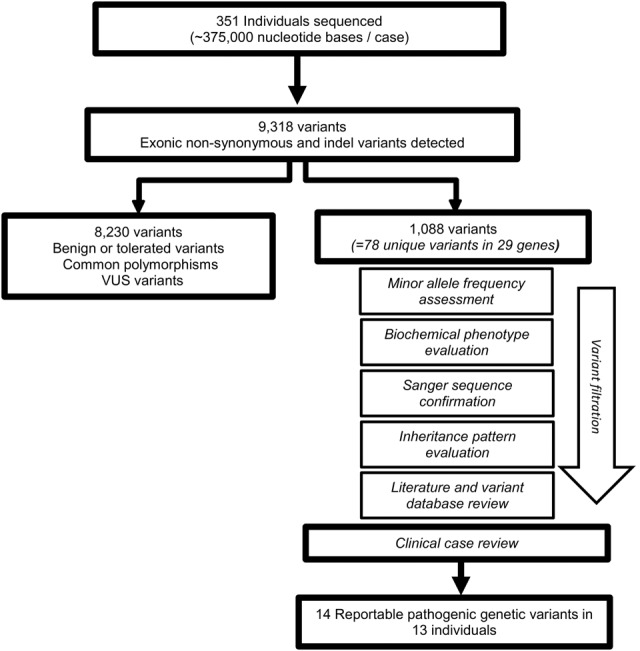
Each year in the United States, thousands of cases of sudden and unexpected deaths of infants, children, and young adults are assigned an undetermined cause of death after postmortem investigation and autopsy. Heritable genetic variants have been suggested as the cause of up to a third of sudden death (SD) cases. Elucidation of the genetic variants involved in SD cases is important to not only help establish cause and manner of death of these individuals, but to also aid in determining whether familial genetic testing should be considered. Previously, these types of postmortem screenings have not been a feasible option for most county medical examiners' and coroners' offices. We sequenced full exons of 64 genes associated with SD in the largest known cohort (351) of infant and young SD decedents using massively parallel sequencing at <$600 per sample. Genetic variants were assessed through literature review and clinical evaluation by a multidisciplinary consortium of experts. Thirteen individuals (3.7%), eight infants (2.8% of those <1 yr of age) and five children/young adults (7.0% of those >1 yr of age), were found to have a reportable genetic variant contributing to SD. These percentages represent an estimate lower than those previously reported. Overall yields and results likely vary between studies due to differences in evaluation techniques and reporting. Additionally, we recommend ongoing assessment of data, including nonreported novel variants, as technology and literature continually advance. This study demonstrates a strategy to implement molecular autopsies in medicolegal investigations of young SD decedents.
© 2016 Methner et al.; Published by Cold Spring Harbor Laboratory Press.
Figures
References
-
- Ackerman MJ. 2005. Cardiac causes of sudden unexpected death in children and their relationship to seizures and syncope: genetic testing for cardiac electropathies. Semin Pediatr Neurol 12: 52–58. - PubMed
-
- Ackerman MJ, Splawski I, Makielski JC, Tester DJ, Will ML, Timothy KW, Keating MT, Jones G, Chadha M, Burrow CR, et al. 2004. Spectrum and prevalence of cardiac sodium channel variants among black, white, Asian, and Hispanic individuals: implications for arrhythmogenic susceptibility and Brugada/long QT syndrome genetic testing. Heart Rhythm 1: 600–607. - PubMed
-
- Ackerman MJ, Priori SG, Willems S, Berul C, Brugada R, Calkins H, Camm AJ, Ellinor PT, Gollob M, Hamilton R, et al. 2011. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies: This document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Europace 13: 1077–1109.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical