

Inflammation and the Intestinal Barrier: Leukocyte-Epithelial Cell Interactions, Cell Junction Remodeling, and Mucosal Repair
- PMID: 27436072
- PMCID: PMC5317033
- DOI: 10.1053/j.gastro.2016.07.008
Inflammation and the Intestinal Barrier: Leukocyte-Epithelial Cell Interactions, Cell Junction Remodeling, and Mucosal Repair
Abstract
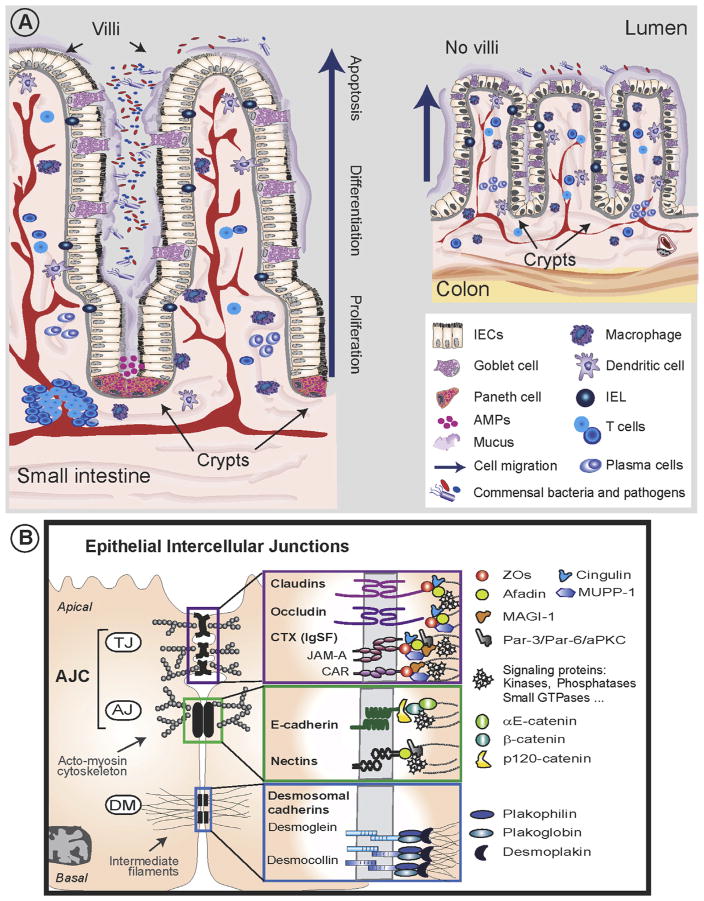
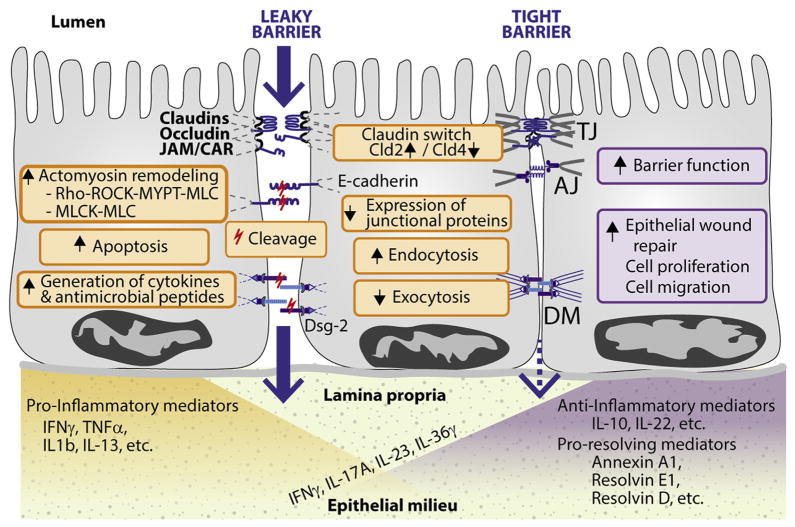
The intestinal tract is lined by a single layer of columnar epithelial cells that forms a dynamic, permeable barrier allowing for selective absorption of nutrients, while restricting access to pathogens and food-borne antigens. Precise regulation of epithelial barrier function is therefore required for maintaining mucosal homeostasis and depends, in part, on barrier-forming elements within the epithelium and a balance between pro- and anti-inflammatory factors in the mucosa. Pathologic states, such as inflammatory bowel disease, are associated with a leaky epithelial barrier, resulting in excessive exposure to microbial antigens, recruitment of leukocytes, release of soluble mediators, and ultimately mucosal damage. An inflammatory microenvironment affects epithelial barrier properties and mucosal homeostasis by altering the structure and function of epithelial intercellular junctions through direct and indirect mechanisms. We review our current understanding of complex interactions between the intestinal epithelium and immune cells, with a focus on pathologic mucosal inflammation and mechanisms of epithelial repair. We discuss leukocyte-epithelial interactions, as well as inflammatory mediators that affect the epithelial barrier and mucosal repair. Increased knowledge of communication networks between the epithelium and immune system will lead to tissue-specific strategies for treating pathologic intestinal inflammation.
Keywords: Epithelium; Inflammation; Mucosal Barrier; Mucosal Repair.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflicts.
Figures
References
-
- Helander HF, Fandriks L. Surface area of the digestive tract—revisited. Scand J Gastroenterol. 2014;49:681–689. - PubMed
-
- Ordas I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet. 2012;380:1606–1619. - PubMed
-
- Katz KD, Hollander D, Vadheim CM, et al. Intestinal permeability in patients with Crohn’s disease and their healthy relatives. Gastroenterology. 1989;97:927–931. - PubMed
-
- Peeters M, Geypens B, Claus D, et al. Clustering of increased small intestinal permeability in families with Crohn’s disease. Gastroenterology. 1997;113:802–807. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
