

Comprehensive Cardiac Magnetic Resonance for Short-Term Follow-Up in Acute Myocarditis
- PMID: 27436306
- PMCID: PMC5015395
- DOI: 10.1161/JAHA.116.003603
Comprehensive Cardiac Magnetic Resonance for Short-Term Follow-Up in Acute Myocarditis
Abstract
Background: Cardiac magnetic resonance (CMR) can detect inflammatory myocardial alterations in patients suspected of having acute myocarditis. There is limited information regarding the degree of normalization of CMR parameters during the course of the disease and the time window during which quantitative CMR should be most reasonably implemented for diagnostic work-up.
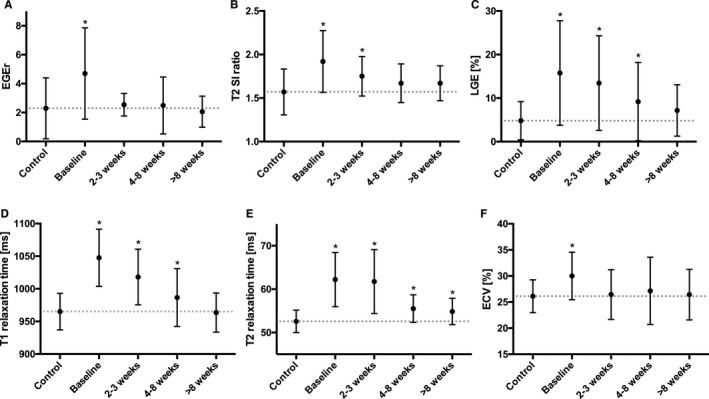
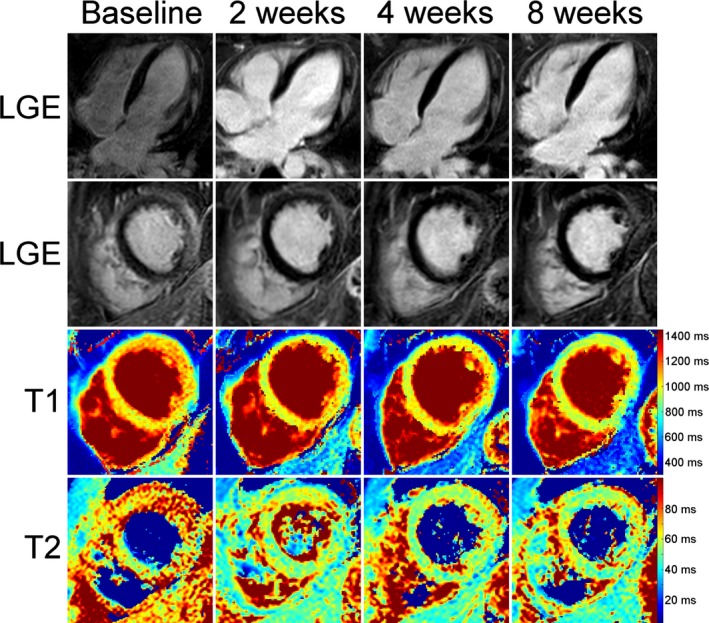
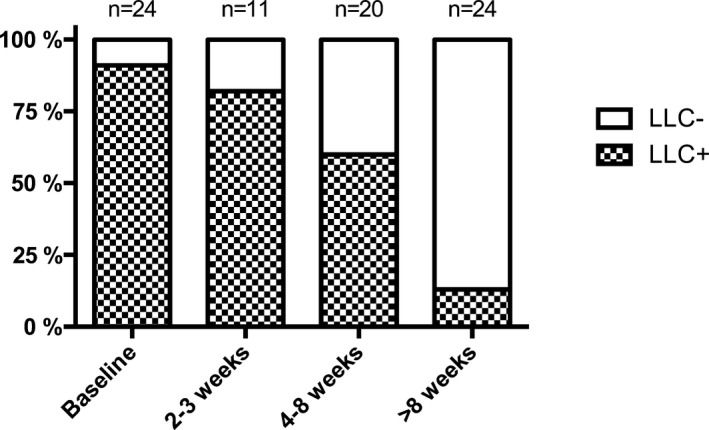
Methods and results: Twenty-four patients with suspected acute myocarditis and 45 control subjects underwent CMR. Initial CMR was performed 2.6±1.9 days after admission. Myocarditis patients underwent CMR follow-up after 2.4±0.6, 5.5±1.3, and 16.2±9.9 weeks. The CMR protocol included assessment of standard Lake Louise criteria, T1 relaxation times, extracellular volume fraction, and T2 relaxation times. Group differences between myocarditis patients and control subjects were highest in the acute stage of the disease (P<0.001 for all parameters). There was a significant and consistent decrease in all inflammatory CMR parameters over the course of the disease (P<0.01 for all parameters). Myocardial T1 and T2 relaxation times-indicative of myocardial edema-were the only single parameters showing significant differences between myocarditis patients and control subjects on 5.5±1.3-week follow-up (T1: 986.5±44.4 ms versus 965.1±28.1 ms, P=0.022; T2: 55.5±3.2 ms versus 52.6±2.6 ms; P=0.001).
Conclusions: In patients with acute myocarditis, CMR markers of myocardial inflammation demonstrated a rapid and continuous decrease over several follow-up examinations. CMR diagnosis of myocarditis should therefore be attempted at an early stage of the disease. Myocardial T1 and T2 relaxation times were the only parameters of active inflammation/edema that could discriminate between myocarditis patients and control subjects even at a convalescent stage of the disease.
Keywords: diagnosis; follow‐up study; magnetic resonance imaging; mapping; myocarditis.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Drory Y, Turetz Y, Hiss Y, Lev B, Fisman EZ, Pines A, Kramer MR. Sudden unexpected death in persons less than 40 years of age. Am J Cardiol. 1991;68:1388–1392. - PubMed
-
- Liu PP, Mason JW. Advances in the understanding of myocarditis. Circulation. 2001;104:1076–1082. - PubMed
-
- Cooper LT, Baughman KL, Feldman AM, Frustaci A, Jessup M, Kuhl U, Levine GN, Narula J, Starling RC, Towbin J, Virmani R; America EbtHFSo, Cardiology tHFAotESo . The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Circulation. 2007;116:2216–2233. - PubMed
-
- Luetkens JA, Homsi R, Sprinkart AM, Doerner J, Dabir D, Kuetting DL, Block W, Andrie R, Stehning C, Fimmers R, Gieseke J, Thomas DK, Schild HH, Naehle CP. Incremental value of quantitative CMR including parametric mapping for the diagnosis of acute myocarditis. Eur Heart J Cardiovasc Imaging. 2016;17:154–161. - PMC - PubMed
-
- Luetkens JA, Doerner J, Thomas DK, Dabir D, Gieseke J, Sprinkart AM, Fimmers R, Stehning C, Homsi R, Schwab JO, Schild H, Naehle CP. Acute myocarditis: multiparametric cardiac MR imaging. Radiology. 2014;273:383–392. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
