

Impact of thoracic radiotherapy timing in limited-stage small-cell lung cancer: usefulness of the individual patient data meta-analysis
- PMID: 27436850
- PMCID: PMC5035783
- DOI: 10.1093/annonc/mdw263
Impact of thoracic radiotherapy timing in limited-stage small-cell lung cancer: usefulness of the individual patient data meta-analysis
Abstract
Background: Chemotherapy (CT) combined with radiotherapy is the standard treatment of 'limited-stage' small-cell lung cancer. However, controversy persists over the optimal timing of thoracic radiotherapy and CT.
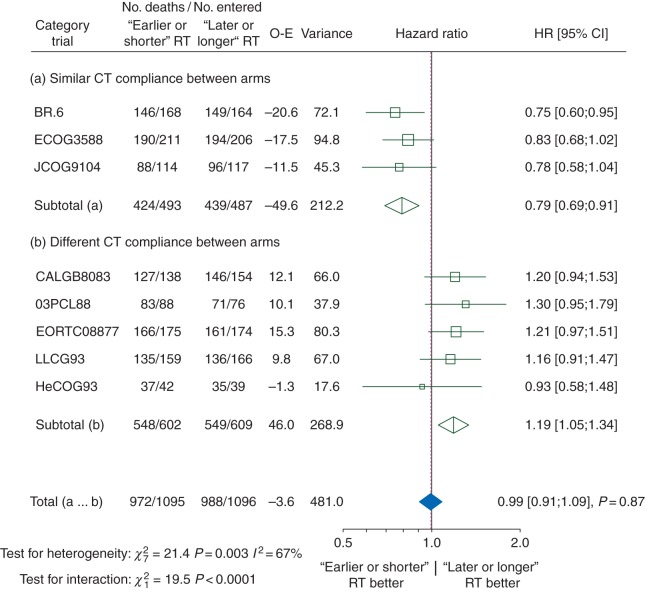
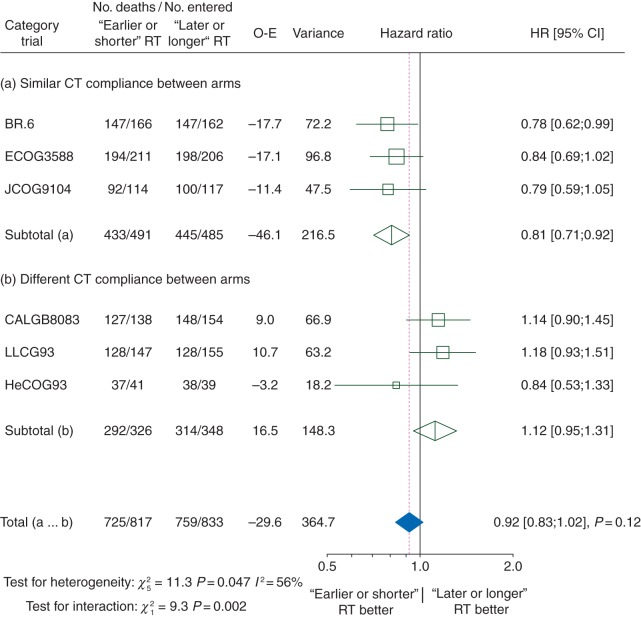
Materials and methods: We carried out a meta-analysis of individual patient data in randomized trials comparing earlier versus later radiotherapy, or shorter versus longer radiotherapy duration, as defined in each trial. We combined the results from trials using the stratified log-rank test to calculate pooled hazard ratios (HRs). The primary outcome was overall survival.
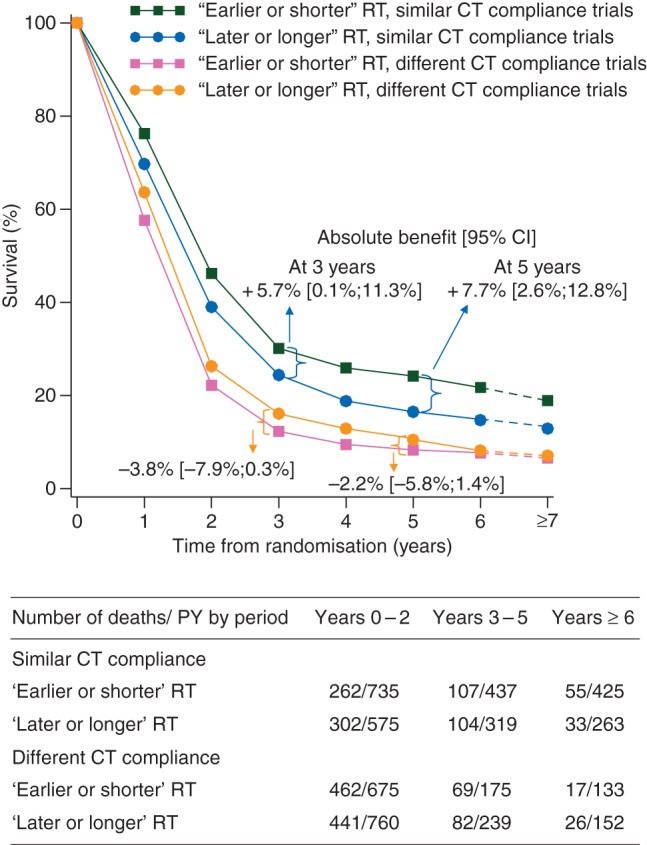
Results: Twelve trials with 2668 patients were eligible. Data from nine trials comprising 2305 patients were available for analysis. The median follow-up was 10 years. When all trials were analysed together, 'earlier or shorter' versus 'later or longer' thoracic radiotherapy did not affect overall survival. However, the HR for overall survival was significantly in favour of 'earlier or shorter' radiotherapy among trials with a similar proportion of patients who were compliant with CT (defined as having received 100% or more of the planned CT cycles) in both arms (HR 0.79, 95% CI 0.69-0.91), and in favour of 'later or longer' radiotherapy among trials with different rates of CT compliance (HR 1.19, 1.05-1.34, interaction test, P < 0.0001). The absolute gain between 'earlier or shorter' versus 'later or longer' thoracic radiotherapy in 5-year overall survival for similar and for different CT compliance trials was 7.7% (95% CI 2.6-12.8%) and -2.2% (-5.8% to 1.4%), respectively. However, 'earlier or shorter' thoracic radiotherapy was associated with a higher incidence of severe acute oesophagitis than 'later or longer' radiotherapy.
Conclusion: 'Earlier or shorter' delivery of thoracic radiotherapy with planned CT significantly improves 5-year overall survival at the expense of more acute toxicity, especially oesophagitis.
Keywords: chemotherapy compliance; individual participant data meta-analysis; radiotherapy timing; randomized clinical trials; small-cell lung cancer; thoracic radiotherapy.
© The Author 2016. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Unresected stage III non-small-cell lung cancer. Provincial Lung Cancer Disease Site Group.Cancer Prev Control. 1997 Aug;1(3):249-59. Cancer Prev Control. 1997. PMID: 9765750
-
Timing of thoracic radiotherapy in limited stage small cell lung cancer: results of early versus late irradiation from a single institution in Turkey.Asian Pac J Cancer Prev. 2014;15(15):6263-7. doi: 10.7314/apjcp.2014.15.15.6263. Asian Pac J Cancer Prev. 2014. PMID: 25124609 Clinical Trial.
-
Randomized phase II trial comparing twice daily hyperfractionated with once daily hypofractionated thoracic radiotherapy in limited disease small cell lung cancer.Acta Oncol. 2016 May;55(5):591-7. doi: 10.3109/0284186X.2015.1092584. Epub 2015 Oct 23. Acta Oncol. 2016. PMID: 26494411 Clinical Trial.
-
Guideline for the Initial Management of Small Cell Lung Cancer (Limited and Extensive Stage) and the Role of Thoracic Radiotherapy and First-line Chemotherapy.Clin Oncol (R Coll Radiol). 2018 Oct;30(10):658-666. doi: 10.1016/j.clon.2018.06.008. Epub 2018 Jul 11. Clin Oncol (R Coll Radiol). 2018. PMID: 30007803
-
Interventions for the treatment of oral and oropharyngeal cancers: surgical treatment.Cochrane Database Syst Rev. 2018 Dec 24;12(12):CD006205. doi: 10.1002/14651858.CD006205.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2023 Aug 31;8:CD006205. doi: 10.1002/14651858.CD006205.pub5. PMID: 30582609 Free PMC article. Updated.
Cited by
-
GOECP/SEOR radiotherapy guidelines for small-cell lung cancer.World J Clin Oncol. 2021 Mar 24;12(3):115-143. doi: 10.5306/wjco.v12.i3.115. World J Clin Oncol. 2021. PMID: 33767969 Free PMC article. Review.
-
Impact of missing individual patient data on 18 meta-analyses of randomised trials in oncology: Gustave Roussy experience.BMJ Open. 2018 Aug 13;8(8):e020499. doi: 10.1136/bmjopen-2017-020499. BMJ Open. 2018. PMID: 30104312 Free PMC article.
-
Immunotherapy in small cell lung cancer: one step at a time: a narrative review.Transl Lung Cancer Res. 2021 Jun;10(6):2970-2987. doi: 10.21037/tlcr-20-630. Transl Lung Cancer Res. 2021. PMID: 34295691 Free PMC article. Review.
-
Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): an open-label, phase 3, randomised, superiority trial.Lancet Oncol. 2017 Aug;18(8):1116-1125. doi: 10.1016/S1470-2045(17)30318-2. Epub 2017 Jun 20. Lancet Oncol. 2017. PMID: 28642008 Free PMC article. Clinical Trial.
-
Optimizing lung cancer radiation treatment worldwide in COVID-19 outbreak.Lung Cancer. 2020 Aug;146:230-235. doi: 10.1016/j.lungcan.2020.05.029. Epub 2020 May 26. Lung Cancer. 2020. PMID: 32585497 Free PMC article. Review.
References
-
- van Meerbeeck JP, Fennell DA, De Ruysscher DK. Small-cell lung cancer. Lancet 2011; 378: 1741–1755. - PubMed
-
- Shepherd FA, Crowley J, Van Houtte P et al. , International Association for the Study of Lung Cancer International Staging Committee and Participating Institutions. The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. J Thorac Oncol 2007; 2: 1067–1077. - PubMed
-
- Arriagada R, Le Chevalier T, Pignon JP et al. . Initial chemotherapy doses and survival in limited small cell lung cancer. N Engl J Med 1993; 329: 1848–1852. - PubMed
-
- Pignon JP, Arriagada R, Ihde DC et al. . A meta-analysis of thoracic radiotherapy for small-cell lung cancer. N Engl J Med 1992; 327: 1618–1624. - PubMed
-
- Stahel R, Thatcher N, Fruh M et al. . 1st ESMO Consensus Conference in lung cancer; Lugano 2010: small-cell lung cancer. Ann Oncol 2011; 22: 1973–1980. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
