

Risk score overestimation: the impact of individual cardiovascular risk factors and preventive therapies on the performance of the American Heart Association-American College of Cardiology-Atherosclerotic Cardiovascular Disease risk score in a modern multi-ethnic cohort
- PMID: 27436865
- PMCID: PMC5837662
- DOI: 10.1093/eurheartj/ehw301
Risk score overestimation: the impact of individual cardiovascular risk factors and preventive therapies on the performance of the American Heart Association-American College of Cardiology-Atherosclerotic Cardiovascular Disease risk score in a modern multi-ethnic cohort
Abstract
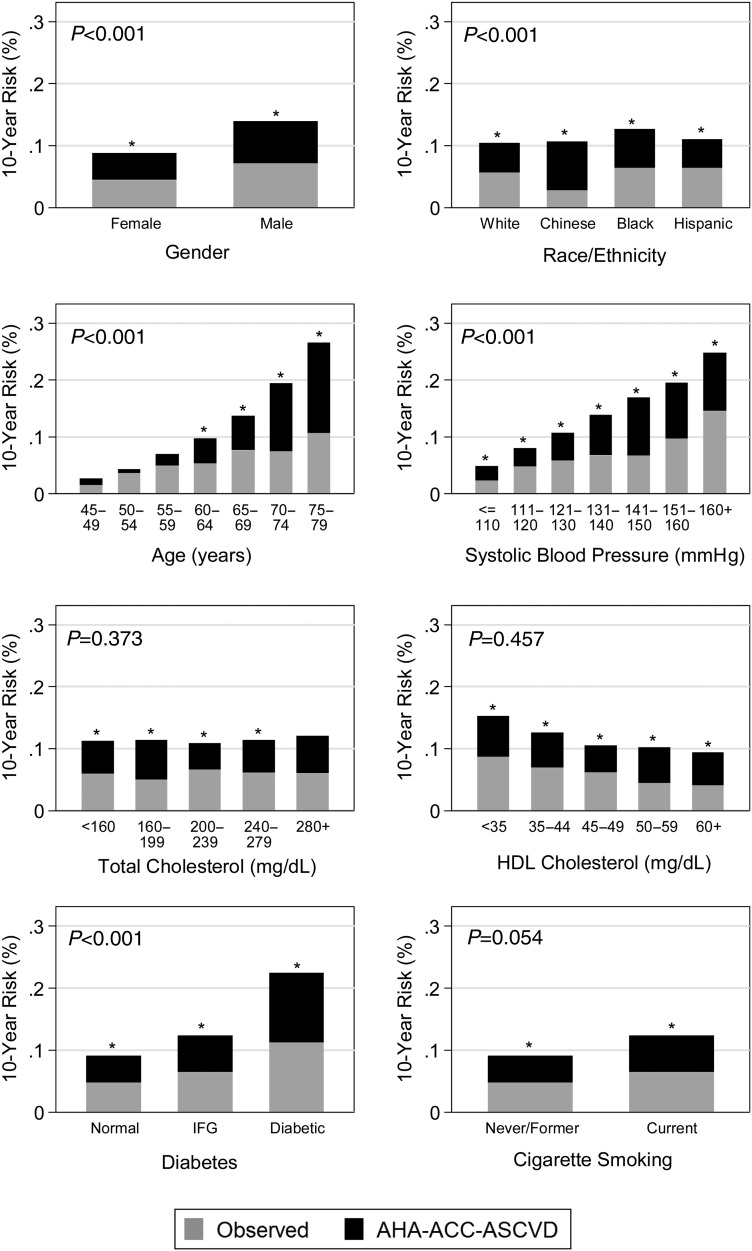
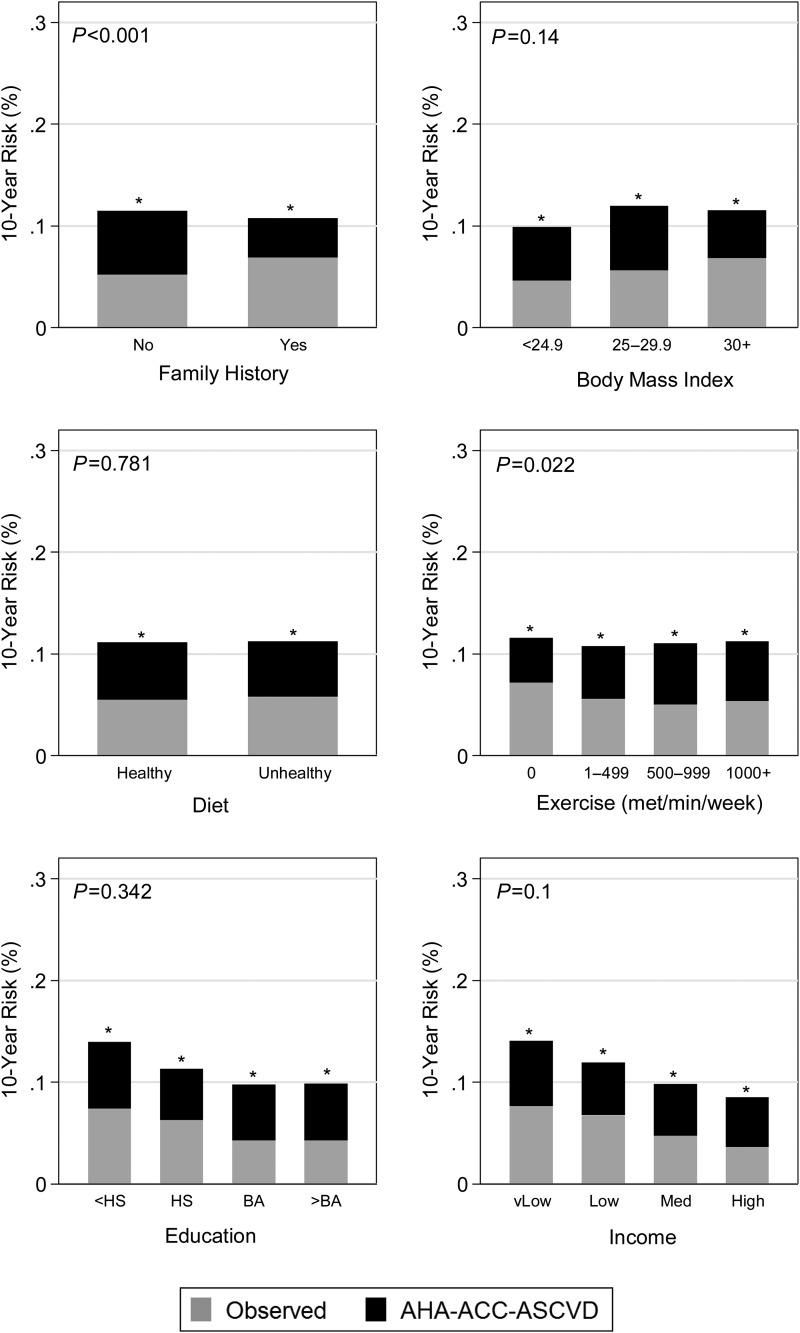
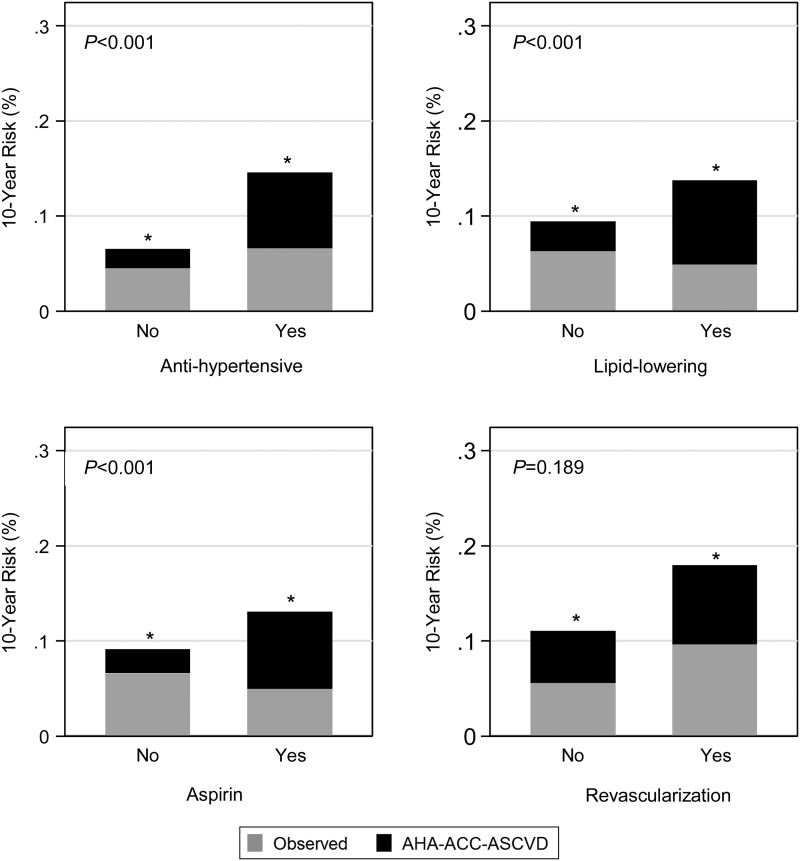
Aims: To evaluate the 2013 American Heart Association (AHA)-American College of Cardiology (ACC)-Atherosclerotic Cardiovascular Disease (ASCVD) risk score among four different race/ethnic groups and to ascertain which factors are most associated with risk overestimation by the AHA-ACC-ASCVD score.
Methods and results: The Multi-Ethnic Study of Atherosclerosis (MESA), a prospective community-based cohort, was used to examine calibration and discrimination of the AHA-ACC-ASCVD risk score in 6441 White, Black, Chinese, and Hispanic Americans (aged 45-79 years and free of known ASCVD at baseline). Using univariable and multivariable absolute risk regression, we modelled the impact of individual risk factors on the discordance between observed and predicted 10-year ASCVD risk. Overestimation was observed in all race/ethnic groups in MESA and was highest among Chinese (252% for women and 314% for men) and lowest in White women (72%) and Hispanic men (67%). Higher age, Chinese race/ethnicity (when compared with White), systolic blood pressure (treated and untreated), diabetes, alcohol use, exercise, lipid-lowering medication, and aspirin use were all associated with more risk overestimation, whereas family history was associated with less risk overestimation in a multivariable model (all P < 0.05).
Conclusion: The AHA-ACC-ASCVD risk score overestimates ASCVD risk among men, women, and all four race/ethnic groups evaluated in a modern American primary prevention cohort. Clinicians treating patients similar to those in MESA, particularly older individuals and those with factors associated with more risk overestimation, may consider interpreting absolute ASCVD risk estimates with caution.
Keywords: Cardiovascular risk prediction; Prevention; Risk factors.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2016. For permissions please email: journals.permissions@oup.com.
Figures
References
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr, Sorlie P, Stone NJ, Wilson PW, Jordan HS, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;129(Suppl. 2):S49–S73. - PubMed
-
- Fried LP, Borhani NO, Enright P, Furberg CD, Gardin JM, Kronmal RA, Kuller LH, Manolio TA, Mittelmark MB, Newman A, O'Leary DH, Psaty B, Rautaharju P, Tracy RP, Weiler PG. The Cardiovascular Health Study: design and rationale. Ann Epidemiol 1991;1:263–276. - PubMed
-
- Friedman GD, Cutter GR, Donahue RP, Hughes GH, Hulley SB, Jacobs DR Jr, Liu K, Savage PJ. CARDIA: study design, recruitment, and some characteristics of the examined subjects. J Clin Epidemiol 1988;41:1105–1116. - PubMed
-
- Investigators TA. The Atherosclerosis Risk in Communities (ARIC) Study: design and objectives. Am J Epidemiol 1989;129:687–702. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
