

Validation of Test Performance and Clinical Time Zero for an Electronic Health Record Embedded Severe Sepsis Alert
- PMID: 27437061
- PMCID: PMC4941860
- DOI: 10.4338/ACI-2015-11-RA-0159
Validation of Test Performance and Clinical Time Zero for an Electronic Health Record Embedded Severe Sepsis Alert
Abstract
Bachground: Increasing use of EHRs has generated interest in the potential of computerized clinical decision support to improve treatment of sepsis. Electronic sepsis alerts have had mixed results due to poor test characteristics, the inability to detect sepsis in a timely fashion and the use of outside software limiting widespread adoption. We describe the development, evaluation and validation of an accurate and timely severe sepsis alert with the potential to impact sepsis management.
Objective: To develop, evaluate, and validate an accurate and timely severe sepsis alert embedded in a commercial EHR.
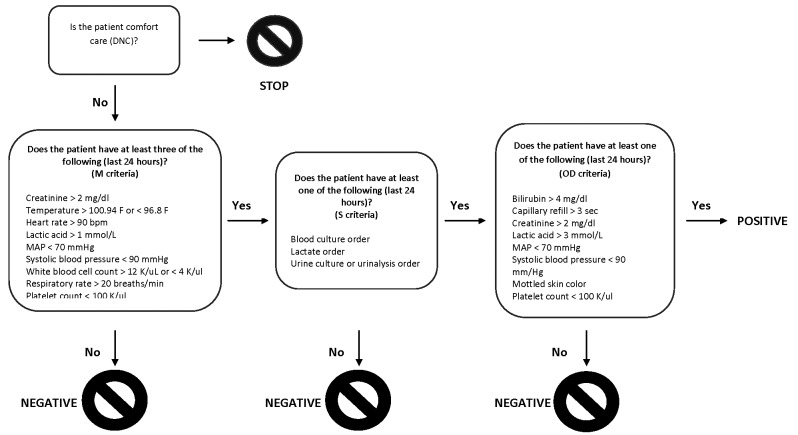
Methods: The sepsis alert was developed by identifying the most common severe sepsis criteria among a cohort of patients with ICD 9 codes indicating a diagnosis of sepsis. This alert requires criteria in three categories: indicators of a systemic inflammatory response, evidence of suspected infection from physician orders, and markers of organ dysfunction. Chart review was used to evaluate test performance and the ability to detect clinical time zero, the point in time when a patient develops severe sepsis.
Results: Two physicians reviewed 100 positive cases and 75 negative cases. Based on this review, sensitivity was 74.5%, specificity was 86.0%, the positive predictive value was 50.3%, and the negative predictive value was 94.7%. The most common source of end-organ dysfunction was MAP less than 70 mm/Hg (59%). The alert was triggered at clinical time zero in 41% of cases and within three hours in 53.6% of cases. 96% of alerts triggered before a manual nurse screen.
Conclusion: We are the first to report the time between a sepsis alert and physician chart-review clinical time zero. Incorporating physician orders in the alert criteria improves specificity while maintaining sensitivity, which is important to reduce alert fatigue. By leveraging standard EHR functionality, this alert could be implemented by other healthcare systems.
Keywords: Testing and evaluation; clinical decision support; inpatient care; medicine; performance improvement.
Conflict of interest statement
The authors declare that they have no conflicts of interest in the research
Figures
Similar articles
-
Diagnostic accuracy of a screening electronic alert tool for severe sepsis and septic shock in the emergency department.BMC Med Inform Decis Mak. 2014 Dec 5;14:105. doi: 10.1186/s12911-014-0105-7. BMC Med Inform Decis Mak. 2014. PMID: 25476738 Free PMC article.
-
Electronic health record-based clinical decision support alert for severe sepsis: a randomised evaluation.BMJ Qual Saf. 2019 Sep;28(9):762-768. doi: 10.1136/bmjqs-2018-008765. Epub 2019 Mar 14. BMJ Qual Saf. 2019. PMID: 30872387 Free PMC article. Clinical Trial.
-
Early Identification of Severe Sepsis in Pediatric Patients Using an Electronic Alert System.Hosp Pediatr. 2023 Feb 1;13(2):174-182. doi: 10.1542/hpeds.2022-006587. Hosp Pediatr. 2023. PMID: 36695040
-
Sepsis Alerts in Emergency Departments: A Systematic Review of Accuracy and Quality Measure Impact.West J Emerg Med. 2020 Aug 24;21(5):1201-1210. doi: 10.5811/westjem.2020.5.46010. West J Emerg Med. 2020. PMID: 32970576 Free PMC article.
-
Development and Implementation of Sepsis Alert Systems.Clin Chest Med. 2016 Jun;37(2):219-29. doi: 10.1016/j.ccm.2016.01.004. Epub 2016 Feb 20. Clin Chest Med. 2016. PMID: 27229639 Free PMC article. Review.
Cited by
-
Evaluation of a Sepsis Alert in the Pediatric Acute Care Setting.Appl Clin Inform. 2021 May;12(3):469-478. doi: 10.1055/s-0041-1730027. Epub 2021 May 26. Appl Clin Inform. 2021. PMID: 34041734 Free PMC article.
-
Visualizing Infection Surveillance Data for Policymaking Using Open Source Dashboarding.Appl Clin Inform. 2019 May;10(3):534-542. doi: 10.1055/s-0039-1693649. Epub 2019 Jul 24. Appl Clin Inform. 2019. PMID: 31340399 Free PMC article.
-
Association of Antibiotics Administration Timing With Mortality in Children With Sepsis in a Tertiary Care Hospital of a Developing Country.Front Pediatr. 2020 Sep 9;8:566. doi: 10.3389/fped.2020.00566. eCollection 2020. Front Pediatr. 2020. PMID: 33014945 Free PMC article.
-
Influencing outcomes with automated time zero for sepsis through statistical validation and process improvement.Mhealth. 2019 Sep 17;5:36. doi: 10.21037/mhealth.2019.09.04. eCollection 2019. Mhealth. 2019. PMID: 31620463 Free PMC article.
-
Information Technology and Acute Kidney Injury: Alerts, Alarms, Bells, and Whistles.Adv Chronic Kidney Dis. 2017 Jul;24(4):241-245. doi: 10.1053/j.ackd.2017.05.007. Adv Chronic Kidney Dis. 2017. PMID: 28778364 Free PMC article. Review.
References
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med 2013; 41(5):1167–1174. - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, Shofer FS, Goyal M. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med 2010; 38(4):1045–1053. - PubMed
-
- Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Horton JM, Studnek JR, Kline JA, Jones AE, Emergency Medicine Shock Research Network (EMSHOCKNET). Association between timing of antibiotic administration and mortality from septic shock in patients treated with a quantitative resuscitation protocol. Crit Care Med 2011; 39(9):2066–2071. - PMC - PubMed
-
- Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker MM, Gerlach H, Reinhart K, Silva E, Harvey M, Regan S, Angus DC. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med 2010; 36(2):222–231. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
