

Incidence and Determinants of Traumatic Intracranial Bleeding Among Older Veterans Receiving Warfarin for Atrial Fibrillation
- PMID: 27437657
- PMCID: PMC5600874
- DOI: 10.1001/jamacardio.2015.0345
Incidence and Determinants of Traumatic Intracranial Bleeding Among Older Veterans Receiving Warfarin for Atrial Fibrillation
Abstract
Importance: Traumatic intracranial bleeding, which is most commonly attributable to falls, is a common concern among health care professionals, who are hesitant to prescribe oral anticoagulants to older adults with atrial fibrillation.
Objective: To describe the incidence of and risk factors for traumatic intracranial bleeding in a large cohort of older adults who were newly prescribed warfarin sodium.
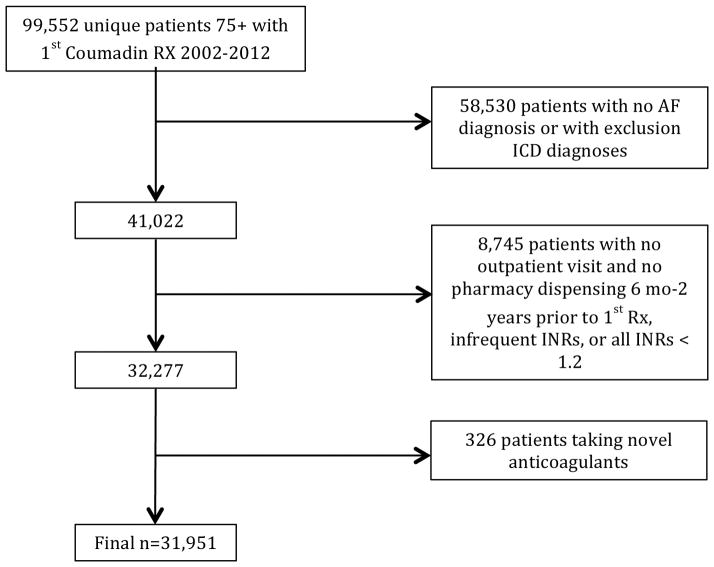
Design, setting, and participants: Retrospective cohort study at the US Department of Veterans Affairs (VA). Participants included 31 951 veterans with atrial fibrillation 75 years or older who were new referrals to VA anticoagulation clinics (for warfarin therapy) between January 1, 2002, and December 31, 2012. The dates of the core analysis were March 2014 through May 2015, and subsequent ad hoc analyses were performed through December 2015. Patients with comorbid conditions requiring warfarin were excluded.
Main outcomes and measures: The primary outcome was hospitalization for traumatic intracranial bleeding. Secondary outcomes included hospitalization for any intracranial bleeding or ischemic stroke. We used International Classification of Diseases, Ninth Revision, Clinical Modification codes to identify the incidence rates of these outcomes after warfarin initiation using VA administrative data (in-system hospitalizations) and Medicare fee-for-service claims data (out-of-system hospitalizations). Clinical characteristics, laboratory results, and pharmacy data were extracted from the VA electronic medical record. For traumatic intracranial bleeding, Cox proportional hazards regression was used to determine predictors of interest selected a priori based on prior known associations.
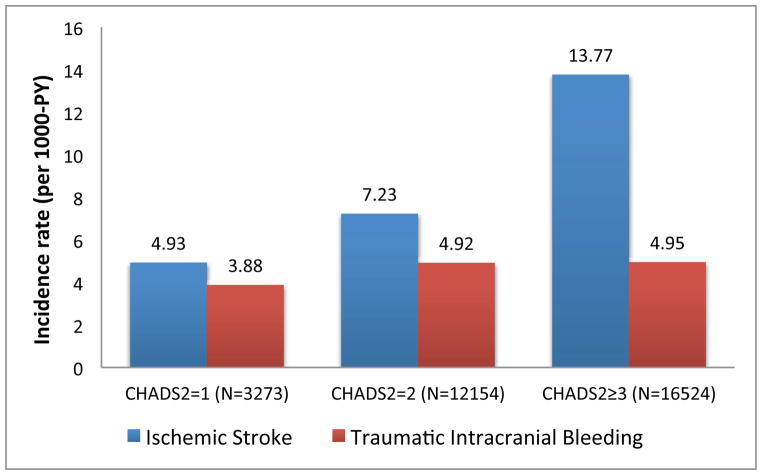
Results: The study population comprised 31 951 participants. The mean (SD) patient age was 81.1 (4.1) years, and 98.1% were male. Comorbidities were common, including hypertension (82.5%), coronary artery disease (42.6%), and diabetes mellitus (33.8%). During the study period, the incidence rate of hospitalization for traumatic intracranial bleeding was 4.80 per 1000 person-years. In unadjusted models, significant predictors of traumatic intracranial bleeding included dementia, fall within the past year, anemia, depression, abnormal renal or liver function, anticonvulsant use, labile international normalized ratio, and antihypertensive use. After adjusting for potential confounders, the remaining significant predictors for traumatic intracranial bleeding were dementia (hazard ratio [HR], 1.76; 95% CI, 1.26-2.46), anemia (HR, 1.23; 95% CI, 1.00-1.52), depression (HR, 1.30; 95% CI, 1.05-1.61), anticonvulsant use (HR, 1.35; 95% CI, 1.04-1.75), and labile international normalized ratio (HR, 1.33; 95% CI, 1.04-1.72). The incidence rates of hospitalization for any intracranial bleeding and ischemic stroke were 14.58 and 13.44, respectively, per 1000 person-years.
Conclusions and relevance: Among patients 75 years or older with atrial fibrillation initiating warfarin therapy, the risk factors for traumatic intracranial bleeding are unique from those for ischemic stroke. The high overall rate of intracranial bleeding in our sample supports the need to more systematically evaluate the benefits and harms of warfarin therapy in older adults.
Figures
Comment in
-
Effect of Drug Interactions and Adherence on Coagulation Control of Patients Treated With Warfarin.JAMA Cardiol. 2016 Oct 1;1(7):849-850. doi: 10.1001/jamacardio.2016.2310. JAMA Cardiol. 2016. PMID: 27556907 No abstract available.
-
Effect of Drug Interactions and Adherence to Warfarin Therapy on Patients-Reply.JAMA Cardiol. 2016 Oct 1;1(7):850. doi: 10.1001/jamacardio.2016.2313. JAMA Cardiol. 2016. PMID: 27557090 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: the anticoagulation and risk factors in atrial fibrillation (ATRIA) study. JAMA. 2001;285(18):2370–2375. - PubMed
-
- Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: Results from the National Registry of Atrial Fibrillation. JAMA. 2001;285(22):2864–2870. - PubMed
-
- Antani MR, Beyth RJ, Covinsky KE, et al. Failure to prescribe warfarin to patients with nonrheumatic atrial fibrillation. J Gen Intern Med. 1996;11(12):713–720. - PubMed
-
- Beyth RJ, Antani MR, Covinsky KE, et al. Why isn’t warfarin prescribed to patients with nonrheumatic atrial fibrillation? J Gen Intern Med. 1996;11(12):721–728. - PubMed
-
- Glader E, Sjölander M, Eriksson M, Lundberg M. Persistent use of secondary preventive drugs declines rapidly during the first 2 years after stroke. Stroke. 2010;41:397–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
