

Resuscitation Practices Associated With Survival After In-Hospital Cardiac Arrest: A Nationwide Survey
- PMID: 27437890
- PMCID: PMC5745254
- DOI: 10.1001/jamacardio.2016.0073
Resuscitation Practices Associated With Survival After In-Hospital Cardiac Arrest: A Nationwide Survey
Erratum in
-
Coding Errors in Survey Study.JAMA Cardiol. 2018 Sep 1;3(9):898. doi: 10.1001/jamacardio.2018.2189. JAMA Cardiol. 2018. PMID: 30046822 Free PMC article. No abstract available.
Abstract
Importance: Although survival of patients with in-hospital cardiac arrest varies markedly among hospitals, specific resuscitation practices that distinguish sites with higher cardiac arrest survival rates remain unknown.
Objective: To identify resuscitation practices associated with higher rates of in-hospital cardiac arrest survival.
Design, setting, and participants: Nationwide survey of resuscitation practices at hospitals participating in the Get With the Guidelines-Resuscitation registry and with 20 or more adult in-hospital cardiac arrest cases from January 1, 2012, through December 31, 2013. Data analysis was performed from June 10 to December 22, 2015.
Main outcomes and measures: Risk-standardized survival rates for cardiac arrest were calculated at each hospital and were then used to categorize hospitals into quintiles of performance. The association between resuscitation practices and quintiles of survival was evaluated using hierarchical proportional odds logistic regression models.
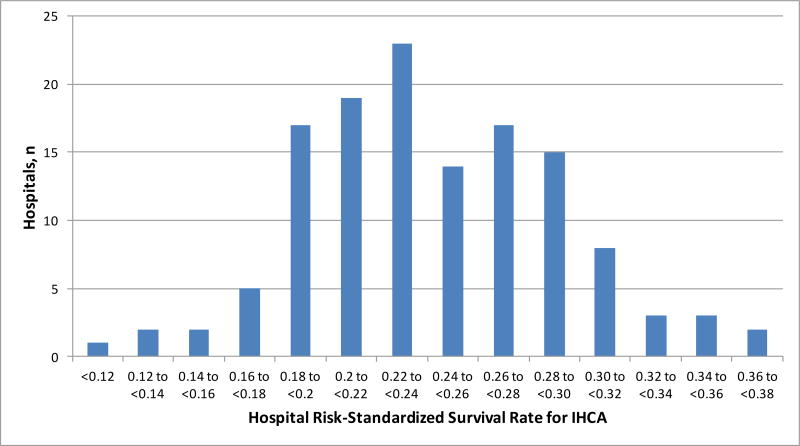
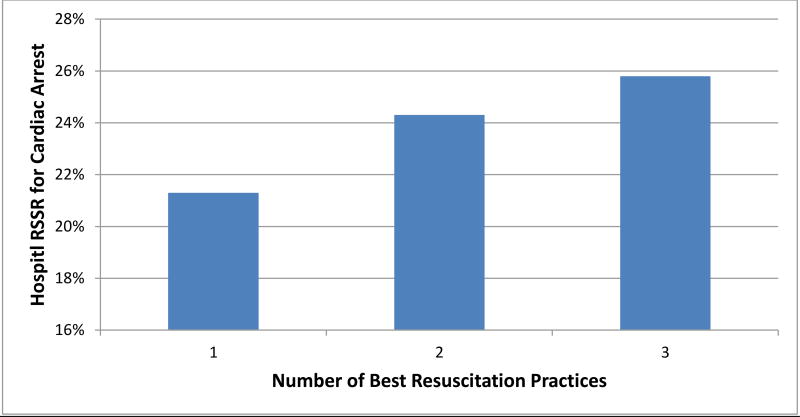
Results: Overall, 150 (78.1%) of 192 eligible hospitals completed the study survey, and 131 facilities with 20 or more adult in-hospital cardiac arrest cases comprised the final study cohort. Risk-standardized survival rates after in-hospital cardiac arrest varied substantially (median, 23.7%; range, 9.2%-37.5%). Several resuscitation practices were associated with survival on bivariate analysis, although only 3 were significant after multivariable adjustment: monitoring for interruptions in chest compressions (adjusted odds ratio [OR] for being in a higher survival quintile category, 2.71; 95% CI, 1.24-5.93; P = .01), reviewing cardiac arrest cases monthly (adjusted OR for being in a higher survival quintile category, 8.55; 95% CI, 1.79-40.00) or quarterly (OR, 6.85; 95% CI, 1.49-31.30; P = .03), and adequate resuscitation training (adjusted OR, 3.23; 95% CI, 1.21-8.33; P = .02).
Conclusions and relevance: Using survey information from acute care hospitals participating in a national quality improvement registry, we identified 3 resuscitation strategies associated with higher hospital rates of survival for patients with in-hospital cardiac arrest. These strategies can form the foundation for best practices for resuscitation care at hospitals given the high incidence and variation in survival for in-hospital cardiac arrest.
Conflict of interest statement
Figures
Comment in
-
Coding Errors in Survey Study of Best Practices for In-Hospital Cardiac Arrest.JAMA Cardiol. 2018 Sep 1;3(9):891-892. doi: 10.1001/jamacardio.2018.2106. JAMA Cardiol. 2018. PMID: 30046832 No abstract available.
References
-
- Strategies to Improve Cardiac Arrest Survivial: A Time to Act. Institute of Medicine; Washington, D.C.: 2015.
-
- Kirkbright S, Finn J, Tohira H, Bremner A, Jacobs I, Celenza A. Audiovisual feedback device use by health care professionals during CPR: a systematic review and meta-analysis of randomised and non-randomised trials. Resuscitation. 2014;85:460–471. - PubMed
-
- Edelson DP, Litzinger B, Arora V, et al. Improving in-hospital cardiac arrest process and outcomes with performance debriefing. Arch Intern Med. 2008;168:1063–1069. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
