

Establishment and antitumor effects of dasatinib and PKI-587 in BD-138T, a patient-derived muscle invasive bladder cancer preclinical platform with concomitant EGFR amplification and PTEN deletion
- PMID: 27438149
- PMCID: PMC5239502
- DOI: 10.18632/oncotarget.10539
Establishment and antitumor effects of dasatinib and PKI-587 in BD-138T, a patient-derived muscle invasive bladder cancer preclinical platform with concomitant EGFR amplification and PTEN deletion
Abstract
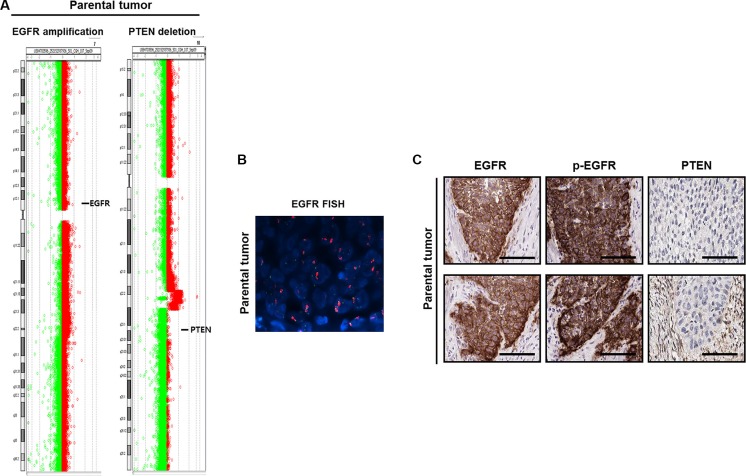
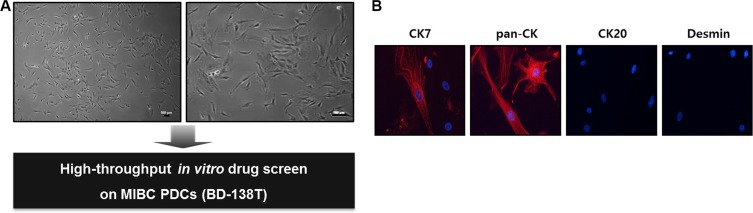
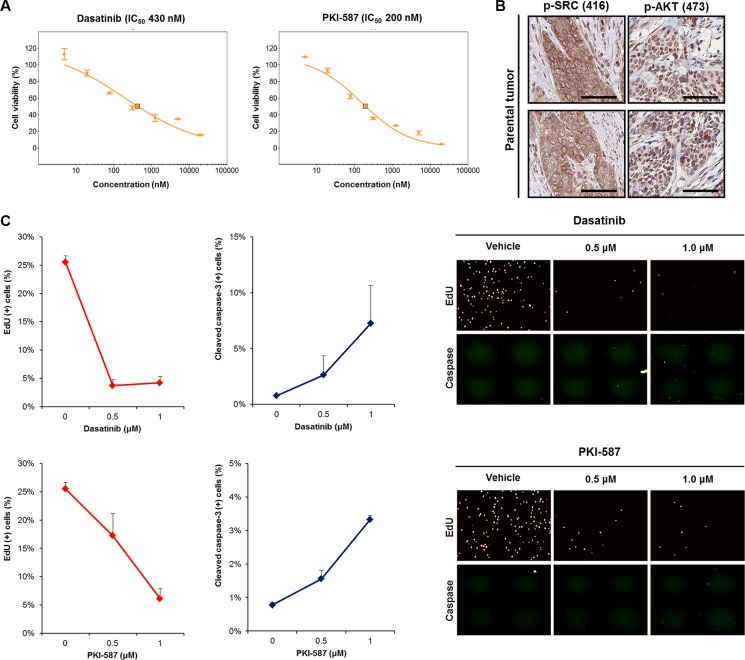
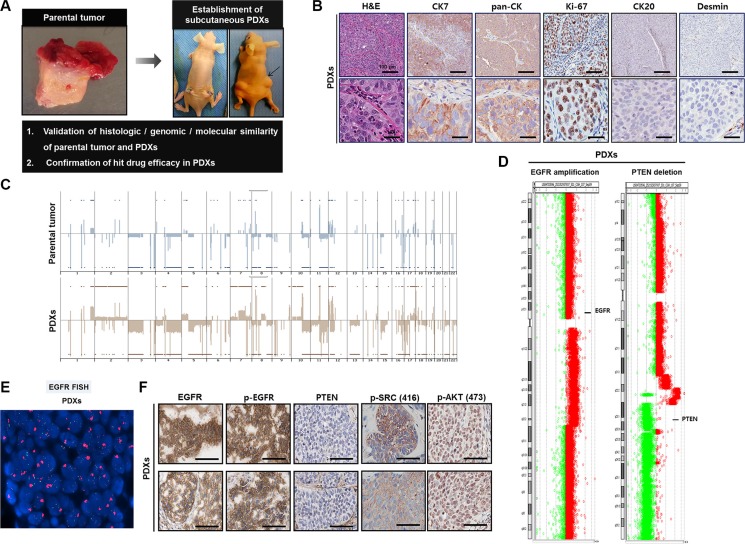
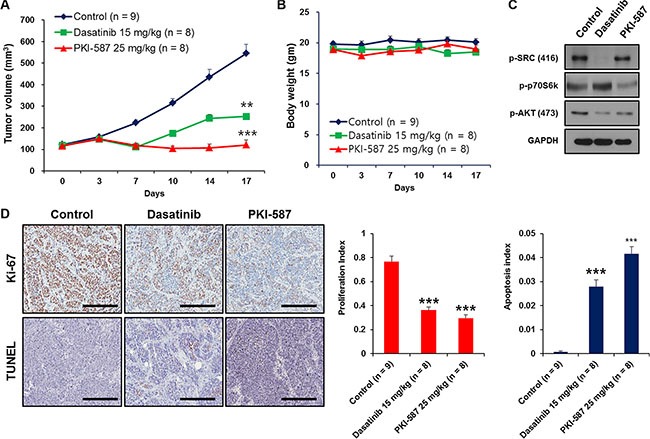
Muscle-invasive bladder cancer (MIBC) consists of a heterogeneous group of tumors with a high rate of metastasis and mortality. To facilitate the in-depth investigation and validation of tailored strategies for MIBC treatment, we have developed an integrated approach using advanced high-throughput drug screening and a clinically relevant patient-derived preclinical platform. We isolated patient-derived tumor cells (PDCs) from a rare MIBC case (BD-138T) that harbors concomitant epidermal growth factor receptor (EGFR) amplification and phosphatase and tensin homolog (PTEN) deletion. High-throughput in vitro drug screening demonstrated that dasatinib, a SRC inhibitor, and PKI-587, a dual PI3K/mTOR inhibitor, exhibited targeted anti-proliferative and pro-apoptotic effects against BD-138T PDCs. Using established patient-derived xenograft models that successfully retain the genomic and molecular characteristics of the parental tumor, we confirmed that these anti-tumor responses occurred through the inhibition of SRC and PI3K/AKT/mTOR signaling pathways. Taken together, these experimental results demonstrate that dasatinib and PKI-587 might serve as promising anticancer drug candidates for treating MIBC with combined EGFR gene amplification and PTEN deletion.
Keywords: EGFR; PTEN; drug screening; muscle invasive bladder cancer; patient-derived xenograft.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflicts of interest.
Figures

References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Zachos I, Konstantinopoulos PA, Tzortzis V, Gravas S, Karatzas A, Karamouzis MV, Melekos M, Papavassiliou AG. Systemic therapy of metastatic bladder cancer in the molecular era: current status and future promise. Expert Opin Investig Drugs. 2010;19:875–887. - PubMed
-
- Wu XR. Urothelial tumorigenesis: a tale of divergent pathways. Nat Rev Cancer. 2005;5:713–725. - PubMed
-
- Cordon-Cardo C. Molecular alterations associated with bladder cancer initiation and progression. Scand J Urol Nephrol Suppl. 2008:154–165. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
