

Predictors of CT Radiation Dose and Their Effect on Patient Care: A Comprehensive Analysis Using Automated Data
- PMID: 27438166
- PMCID: PMC5207127
- DOI: 10.1148/radiol.2016151391
Predictors of CT Radiation Dose and Their Effect on Patient Care: A Comprehensive Analysis Using Automated Data
Abstract
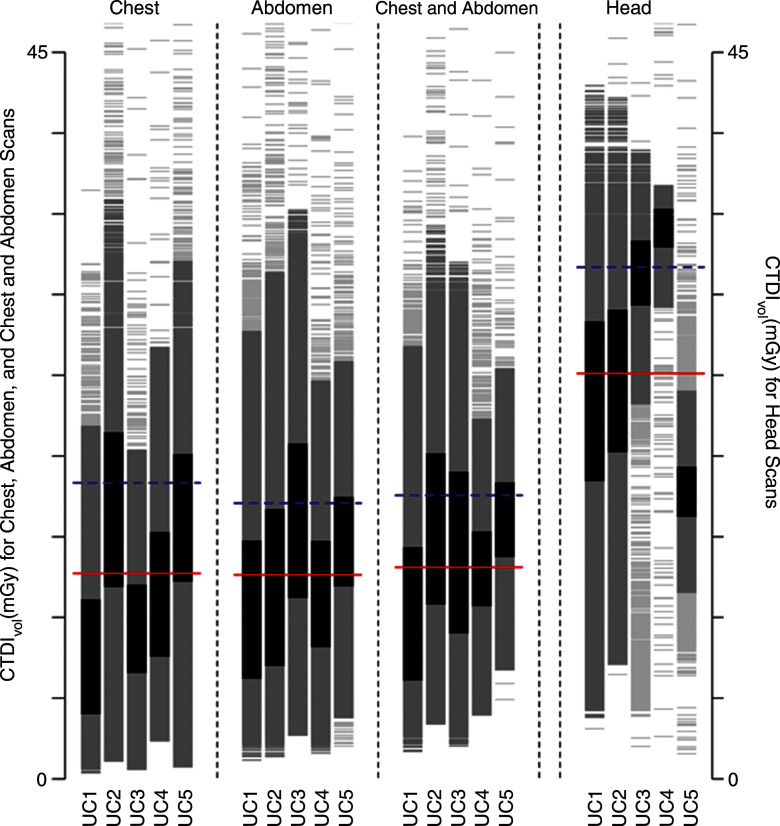
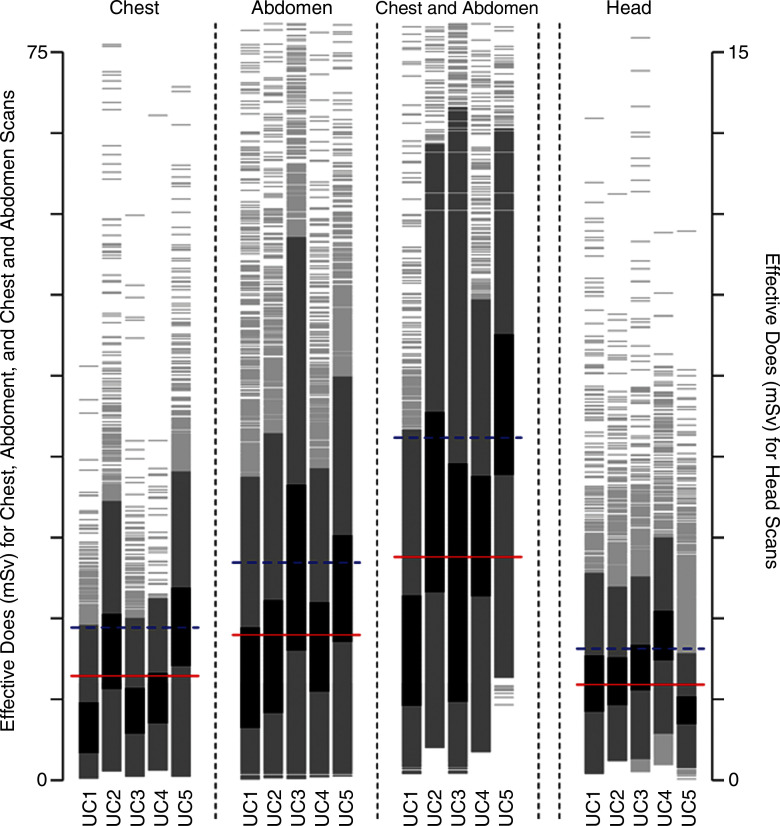
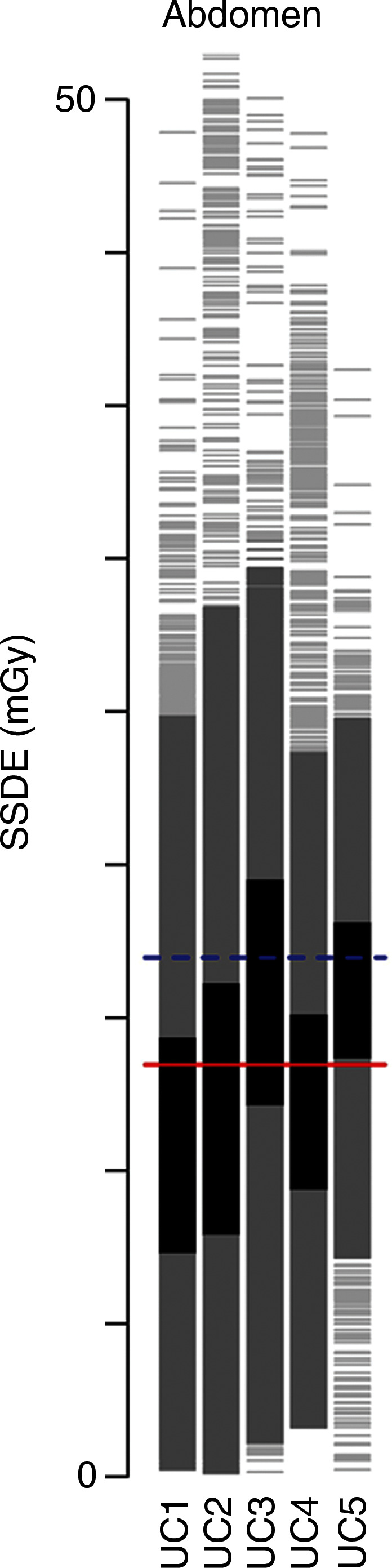
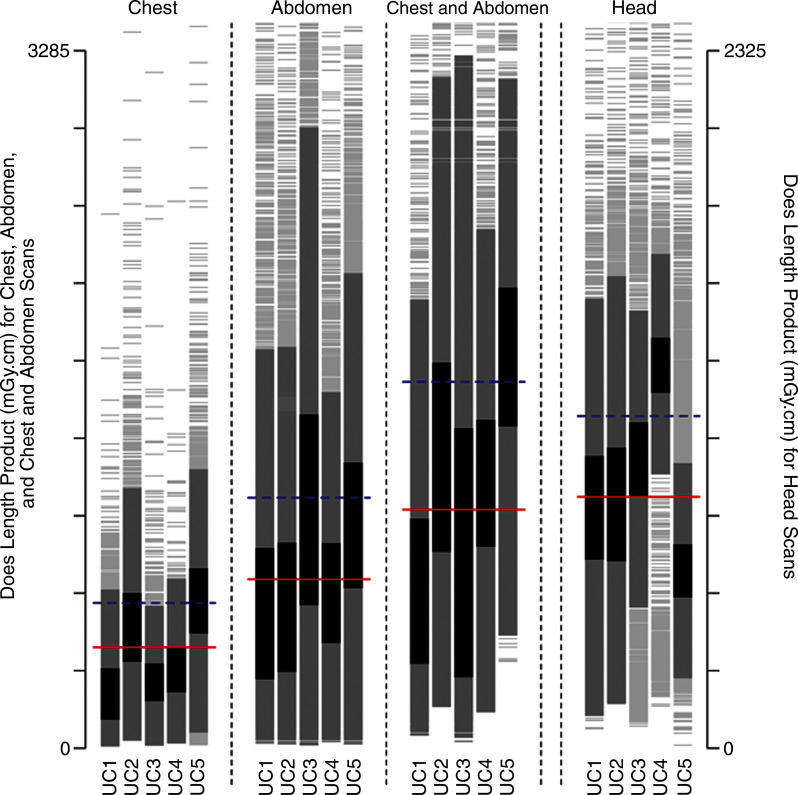
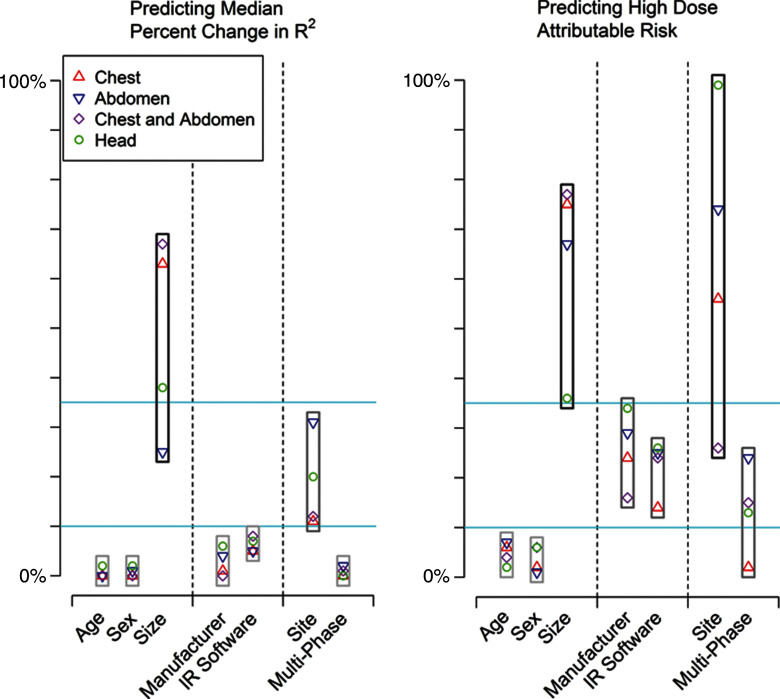
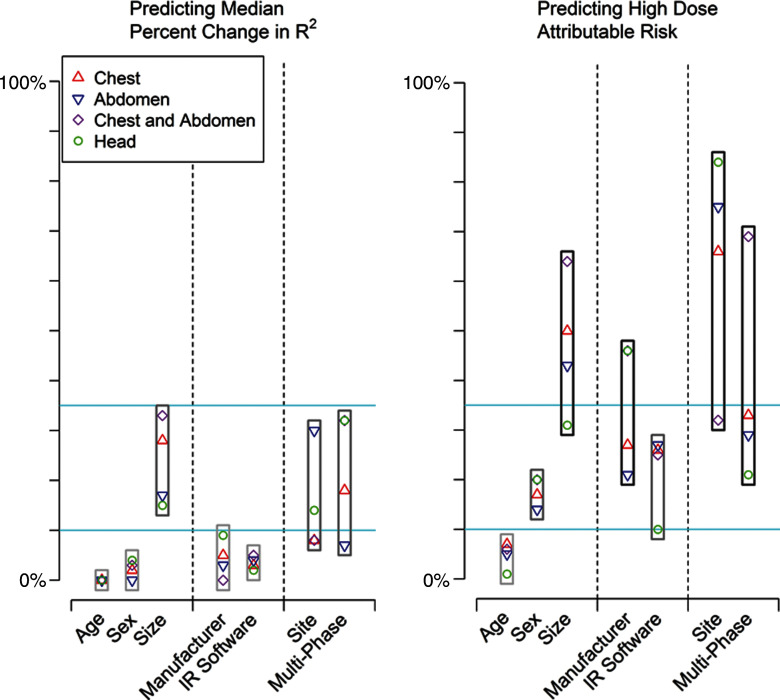
Purpose To determine patient, vendor, and institutional factors that influence computed tomography (CT) radiation dose. Materials and Methods The relevant institutional review boards approved this HIPAA-compliant study, with waiver of informed consent. Volume CT dose index (CTDIvol) and effective dose in 274 124 head, chest, and abdominal CT examinations performed in adult patients at 12 facilities in 2013 were collected prospectively. Patient, vendor, and institutional characteristics that could be used to predict (a) median dose by using linear regression after log transformation of doses and (b) high-dose examinations (top 25% of dose within anatomic strata) by using modified Poisson regression were assessed. Results There was wide variation in dose within and across medical centers. For chest CTDIvol, overall median dose across all institutions was 11 mGy, and institutional median dose was 7-16 mGy. Models including patient, vendor, and institutional factors were good for prediction of median doses (R2 = 0.31-0.61). The specific institution where the examination was performed (reflecting the specific protocols used) accounted for a moderate to large proportion of dose variation. For chest CTDIvol, unadjusted median CTDIvol was 16.5 mGy at one institution and 6.7 mGy at another (adjusted relative median dose, 2.6 mGy [95% confidence interval: 2.5, 2.7]). Several variables were important predictors that a patient would undergo high-dose CT. These included patient size, the specific institution where CT was performed, and the use of multiphase scanning. For example, while 49% of patients (21 411 of 43 696) who underwent multiphase abdominal CT had a high-dose examination, 8% of patients (4977 of 62 212) who underwent single-phase CT had a high-dose examination (adjusted relative risk, 6.20 [95% CI: 6.17, 6.23]). If all patients had been examined with single-phase CT, 69% (18 208 of 26 388) of high-dose examinations would have been eliminated. Patient size, institutional-specific protocols, and multiphase scanning were the most important predictors of dose (change in R2 = 8%-32%), followed by manufacturer and iterative reconstruction (change in R2, 0.2%-15.0%). Conclusion CT doses vary considerably within and across facilities. The primary factors that influenced dose variation were multiphase scanning and institutional protocol choices. It is unknown if the variation in these factors influenced diagnostic accuracy. © RSNA, 2016.
Conflict of interest statement
Figures
References
-
- Radimetrics Enterprise Platform. Bayer Web site. https://www.radiologysolutions.bayer.com/products/ct/dosemanagement/rep/. Updated June 2016. Accessed June 29, 2016 .
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
