

Racial Differences in Atrial Fibrillation-Related Cardiovascular Disease and Mortality: The Atherosclerosis Risk in Communities (ARIC) Study
- PMID: 27438320
- PMCID: PMC5347977
- DOI: 10.1001/jamacardio.2016.1025
Racial Differences in Atrial Fibrillation-Related Cardiovascular Disease and Mortality: The Atherosclerosis Risk in Communities (ARIC) Study
Abstract
Importance: The adverse outcomes associated with atrial fibrillation (AF) have been studied in predominantly white cohorts. Racial differences in outcomes associated with AF merit continued investigation.
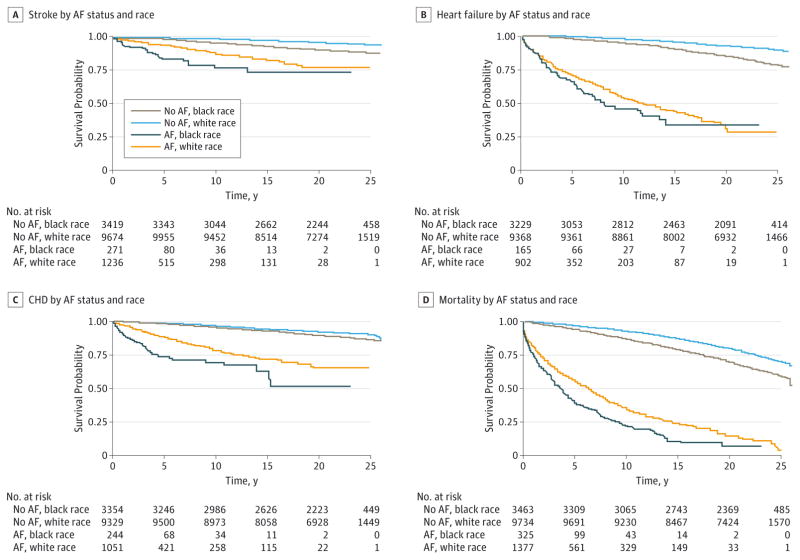
Objective: To evaluate the race-specific associations of AF with stroke, heart failure, coronary heart disease (CHD), and all-cause mortality in a community-based cohort.
Design, setting, and participants: The Atherosclerosis Risk in Communities (ARIC) Study is a prospective, observational cohort. From 1987 through 1989, the ARIC Study enrolled 15 792 men and women and conducted 4 follow-up examinations (2011-2013) with active surveillance for vital status and hospitalizations. Race was determined by self-report and categorized as white, black, or other.
Main outcomes and measures: Atrial fibrillation (adjudicated using electrocardiograms, hospital discharge codes, and death certificates), stroke, heart failure, CHD, and mortality.
Results: After exclusions, 15 080 participants (mean [SD] age, 54.2 [5.8] years; 8290 women [55.5%]; 3831 black individuals [25.4%]) were included in this analysis. During a mean (SD) follow-up of 20.6 (6.2) years, there were 2348 cases of incident AF. The incident rates of AF per 1000 person-years were 8.1 (95% CI, 7.7-8.5) in white individuals and 5.8 (95% CI, 5.2-6.3) in black individuals. The rates of stroke, heart failure, CHD, and mortality were higher in black individuals with AF than white individuals with AF. The association of AF with these outcomes, estimated with rate differences (rate of the end point in those with AF minus the rate in those without AF per 1000 person-years), also differed by race. The rate difference for stroke in individuals with AF was 10.2 (95% CI, 6.6-13.9) in white individuals and 21.4 (95% CI, 10.2-32.6) in black individuals. For heart failure and CHD, the rate differences were 1.5- to 2.0-fold higher in black individuals than white individuals. White individuals with AF had a rate difference of 55.9 (95% CI, 48.1-63.7) for mortality compared with black individuals, who had a rate difference of 106.0 (95% CI, 86.0-125.9).
Conclusions and relevance: In the prospective ARIC Study, the outcome of AF on the rates of stroke, heart failure, CHD, and mortality was considerably larger in black individuals than white individuals. These results indicate the vulnerability and increased risk in black individuals with AF. Continued investigation of racial differences in AF and its related adverse outcomes are essential to identify and mitigate racial disparities in the treatment of AF.
Conflict of interest statement
Figures

Comment in
-
The "Double" Paradox of Atrial Fibrillation in Black Individuals.JAMA Cardiol. 2016 Jul 1;1(4):377-9. doi: 10.1001/jamacardio.2016.1259. JAMA Cardiol. 2016. PMID: 27438310 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the An Ticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370–2375. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22(8):983–988. - PubMed
-
- Wang TJ, Larson MG, Levy D, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107(23):2920–2925. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R01 HL122200/HL/NHLBI NIH HHS/United States
- 2015084/DDCF/Doris Duke Charitable Foundation/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- 16EIA26410001/AHA/American Heart Association-American Stroke Association/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
