

Six-Year Change in High-Sensitivity Cardiac Troponin T and Risk of Subsequent Coronary Heart Disease, Heart Failure, and Death
- PMID: 27439107
- PMCID: PMC5084093
- DOI: 10.1001/jamacardio.2016.0765
Six-Year Change in High-Sensitivity Cardiac Troponin T and Risk of Subsequent Coronary Heart Disease, Heart Failure, and Death
Abstract
Importance: High-sensitivity cardiac troponin T (hs-cTnT) is a biomarker of cardiovascular risk and could be approved in the United States for clinical use soon. However, data linking long-term temporal change in hs-cTnT to outcomes are limited, particularly in primary prevention settings.
Objective: To examine the association of 6-year change in hs-cTnT with incident coronary heart disease (CHD), heart failure (HF), and all-cause mortality.
Design, setting, and participants: This prospective observational cohort study, performed from January 1, 1990, to December 31, 2011, included 8838 participants with biracial representation from the Atherosclerosis Risk in Communities Study who were initially free of CHD and HF and who had hs-cTnT measured twice, 6 years apart. Data analysis was performed from October 28, 2014, to March 9, 2016.
Main outcome and measures: Risk factor and temporal hs-cTnT data were collected. Using Cox proportional hazards regression, we examined the association of hs-cTnT change with subsequent CHD, HF, and death during a maximum of 16 years. Improvement in discrimination was determined by the Harrell C statistic.
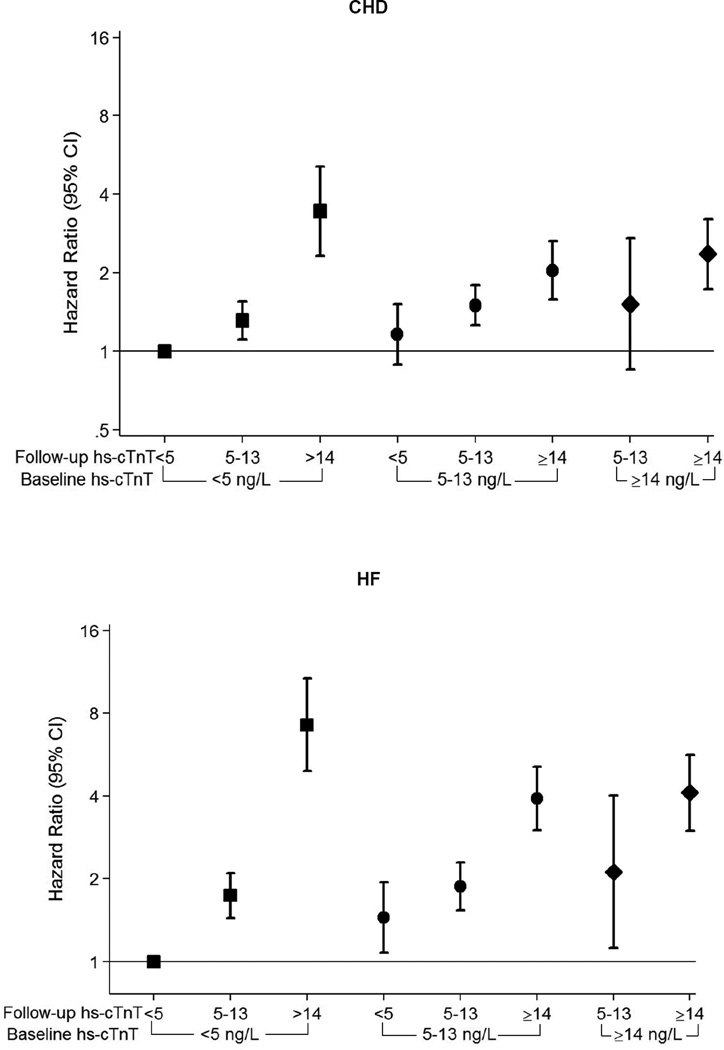
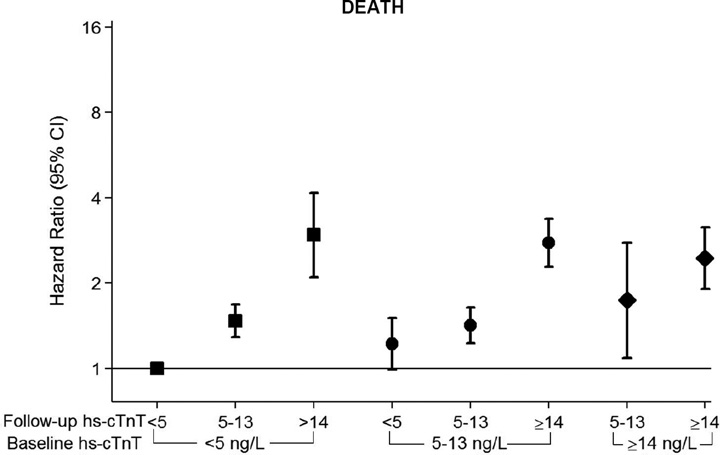
Results: Of the 8838 participants (mean age, 56 years; 5215 female [59.0%]; 1891 black [21.4%]) there were 1157 CHD events, 965 HF events, and 1813 deaths overall. Incident detectable hs-cTnT (baseline, <0.005 ng/mL; follow-up, ≥0.005 ng/mL) was independently associated with subsequent CHD (hazard ratio [HR], 1.4; 95% CI, 1.2-1.6), HF (HR, 2.0; 95% CI, 1.6-2.4), and death (HR, 1.5; 95% CI, 1.3-1.7), relative to an hs-cTnT level less than 0.005 ng/mL at both visits. In addition, HRs as high as 4 for CHD and death and 8 for HF were recorded among individuals with the most marked hs-cTnT increases (eg, baseline, < 0.005 ng/mL; follow-up, ≥0.014 ng/mL). Risk for subsequent outcomes was lower among those with relative hs-cTnT reductions greater than 50% from baseline. Furthermore, information on hs-cTnT change improved discrimination for HF and death when added to a model that included traditional risk factors, N-terminal pro-brain natriuretic peptide, and baseline hs-cTnT level. Among individuals with adjudicated HF hospitalizations, hs-cTnT change appeared to be similarly associated with HF with reduced and preserved ejection fraction.
Conclusions and relevance: Temporal increases in hs-cTnT, suggestive of progressive myocardial damage, are independently associated with incident CHD, death, and, above all, HF. Serial determination of hs-cTnT trajectory adds clinically relevant information to baseline testing and may be useful in prognostic assessments and the targeting of prevention strategies to high-risk individuals, especially among persons with stage A or B HF.
Conflict of interest statement
Disclosures: The other authors declare no commercial conflicts of interest (but receive National Institutes of Health grant funding).
Figures
Comment in
-
Biomarkers to Predict Risk in Apparently Well Populations.JAMA Cardiol. 2016 Aug 1;1(5):528-9. doi: 10.1001/jamacardio.2016.1019. JAMA Cardiol. 2016. PMID: 27438941 No abstract available.
References
-
- Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012 Oct 16;126(16):2020–2035. - PubMed
-
- Apple FS. High-sensitivity cardiac troponin for screening large populations of healthy people: is there risk? Clinical chemistry. 2011 Apr;57(4):537–539. - PubMed
-
- Giannitsis E, Katus HA. Highly sensitive troponins knocking at the door of primary prevention. European heart journal. 2014 Feb;35(5):268–270. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
