

Multiscale Systems-Pharmacology Pipeline to Assess the Prophylactic Efficacy of NRTIs Against HIV-1
- PMID: 27439573
- PMCID: PMC4961081
- DOI: 10.1002/psp4.12095
Multiscale Systems-Pharmacology Pipeline to Assess the Prophylactic Efficacy of NRTIs Against HIV-1
Abstract
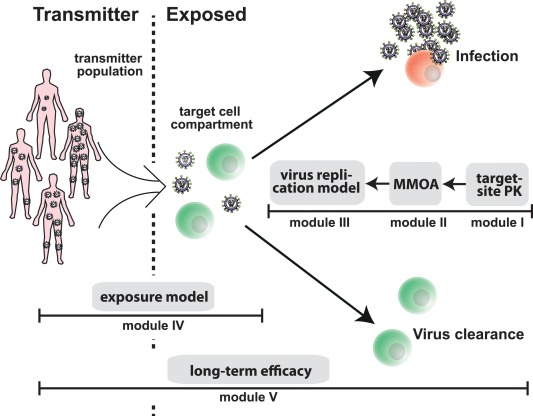
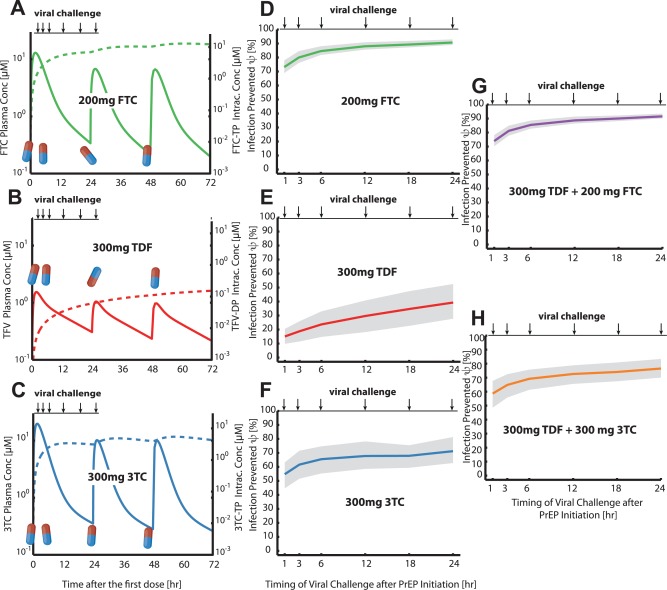
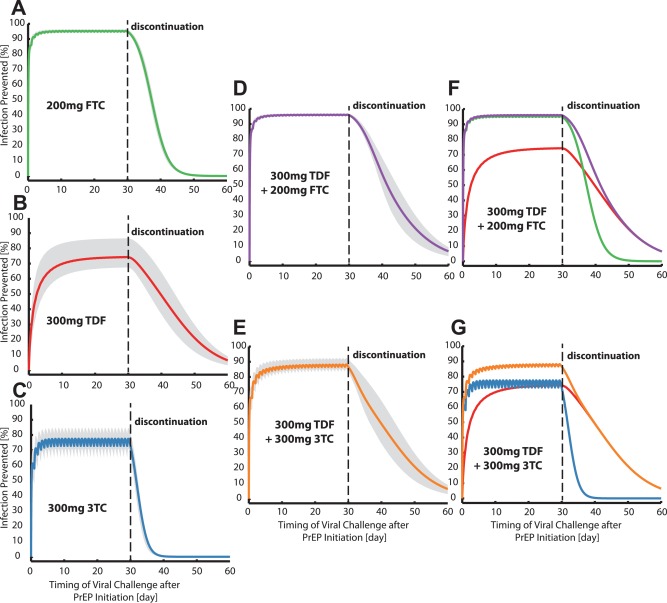
While HIV-1 continues to spread, the use of antivirals in preexposure prophylaxis (PrEP) has recently been suggested. Here we present a modular systems pharmacology modeling pipeline, predicting PrEP efficacy of nucleotide reverse transcriptase inhibitors (NRTIs) at the scale of reverse transcription, target-cell, and systemic infection and after repeated viral exposures, akin to clinical trials. We use this pipeline to benchmark the prophylactic efficacy of all currently approved NRTIs in wildtype and mutant viruses. By integrating pharmacokinetic models, we find that intracellular tenofovir-diphosphate builds up too slowly to halt infection when taken "on demand" and that lamivudine may substitute emtricitabine in PrEP combinations. Lastly, we delineate factors confounding clinical PrEP efficacy estimates and provide a method to overcome these. The presented framework is useful to screen and optimize PrEP candidates and strategies and to understand their clinical efficacy by integrating the diverse scales which determine PrEP efficacy.
© 2016 The Authors CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals, Inc. on behalf of American Society for Clinical Pharmacology and Therapeutics.
Figures

Similar articles
-
Pharmacokinetics and pharmacodynamics of the reverse transcriptase inhibitor tenofovir and prophylactic efficacy against HIV-1 infection.PLoS One. 2012;7(7):e40382. doi: 10.1371/journal.pone.0040382. Epub 2012 Jul 11. PLoS One. 2012. PMID: 22808148 Free PMC article.
-
Top-down and bottom-up modeling in system pharmacology to understand clinical efficacy: An example with NRTIs of HIV-1.Eur J Pharm Sci. 2016 Oct 30;94:72-83. doi: 10.1016/j.ejps.2016.01.016. Epub 2016 Jan 18. Eur J Pharm Sci. 2016. PMID: 26796142
-
The future of pre-exposure prophylaxis (PrEP) for human immunodeficiency virus (HIV) infection.Expert Rev Anti Infect Ther. 2017 May;15(5):467-481. doi: 10.1080/14787210.2017.1309292. Epub 2017 Apr 4. Expert Rev Anti Infect Ther. 2017. PMID: 28322067 Review.
-
Hybrid stochastic framework predicts efficacy of prophylaxis against HIV: An example with different dolutegravir prophylaxis schemes.PLoS Comput Biol. 2018 Jun 14;14(6):e1006155. doi: 10.1371/journal.pcbi.1006155. eCollection 2018 Jun. PLoS Comput Biol. 2018. PMID: 29902179 Free PMC article.
-
Pharmacokinetics of nucleoside/nucleotide reverse transcriptase inhibitors for the treatment and prevention of HIV infection.Expert Opin Drug Metab Toxicol. 2020 Jul;16(7):551-564. doi: 10.1080/17425255.2020.1772755. Epub 2020 Jun 7. Expert Opin Drug Metab Toxicol. 2020. PMID: 32508203 Review.
Cited by
-
Modeling HIV Pre-Exposure Prophylaxis.Front Pharmacol. 2020 Jan 31;10:1514. doi: 10.3389/fphar.2019.01514. eCollection 2019. Front Pharmacol. 2020. PMID: 32082142 Free PMC article. Review.
-
Mathematical Modelling of the Molecular Mechanisms of Interaction of Tenofovir with Emtricitabine against HIV.Viruses. 2021 Jul 13;13(7):1354. doi: 10.3390/v13071354. Viruses. 2021. PMID: 34372560 Free PMC article.
-
Large benefits to youth-focused HIV treatment-as-prevention efforts in generalized heterosexual populations: An agent-based simulation model.PLoS Comput Biol. 2019 Dec 17;15(12):e1007561. doi: 10.1371/journal.pcbi.1007561. eCollection 2019 Dec. PLoS Comput Biol. 2019. PMID: 31846456 Free PMC article.
-
Assessment of Demographic and Socio-Behavioral Factors on Adherence to HIV Pre-Exposure Prophylaxis Using a Markov Modeling Approach.Front Pharmacol. 2019 Jul 12;10:785. doi: 10.3389/fphar.2019.00785. eCollection 2019. Front Pharmacol. 2019. PMID: 31354496 Free PMC article.
-
Numerical approaches for the rapid analysis of prophylactic efficacy against HIV with arbitrary drug-dosing schemes.PLoS Comput Biol. 2021 Dec 23;17(12):e1009295. doi: 10.1371/journal.pcbi.1009295. eCollection 2021 Dec. PLoS Comput Biol. 2021. PMID: 34941864 Free PMC article.
References
-
- Chun, T.W , Moir, S. & Fauci, A.S HIV reservoirs as obstacles and opportunities for an HIV cure. Nat. Immunol. 16, 584–589 (2015). - PubMed
-
- UNAIDS . AIDS by the Numbers 2015. <http://www.unaids.org/en/resources/documents/2015/AIDS_by_the_numbers_2015>. Accessed 31 Mar 2016. Technical report, 2015.
-
- Mouquet, H. & Nussenzweig, M.C. HIV: Roadmaps to a vaccine. Nature 496, 441–442 (2013). - PubMed
-
- Boffito, M. , Jackson, A. & Asboe, D. Pharmacology lessons from chemoprophylaxis studies. Clin. Infect. Dis. 59(supp. 1), S52–S54 (2014). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
