

Motor and Cognitive Functional Status Are Associated with 30-day Unplanned Rehospitalization Following Post-Acute Care in Medicare Fee-for-Service Beneficiaries
- PMID: 27439979
- PMCID: PMC5130938
- DOI: 10.1007/s11606-016-3704-4
Motor and Cognitive Functional Status Are Associated with 30-day Unplanned Rehospitalization Following Post-Acute Care in Medicare Fee-for-Service Beneficiaries
Abstract
Background: The Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014 stipulates that standardized functional status (self-care and mobility) and cognitive function data will be used for quality reporting in post-acute care settings. Thirty-day post-discharge unplanned rehospitalization is an established quality metric that has recently been extended to post-acute settings. The relationships between the functional domains in the IMPACT Act and 30-day unplanned rehospitalization are poorly understood.
Objective: To determine the degree to which discharge mobility, self-care, and cognitive function are associated with 30-day unplanned rehospitalization following discharge from post-acute care.
Design: This was a retrospective cohort study.
Setting: Inpatient rehabilitation facilities submitting claims and assessment data to the Centers for Medicare and Medicaid Services in 2012-2013.
Participants: Medicare fee-for-service enrollees discharged from post-acute rehabilitation in 2012-2013. The sample included community-dwelling adults admitted for rehabilitation following an acute care stay who survived for 32 days following discharge (N = 252,406).
Interventions: Not applicable.
Main measures: Thirty-day unplanned rehospitalization following post-acute rehabilitation.
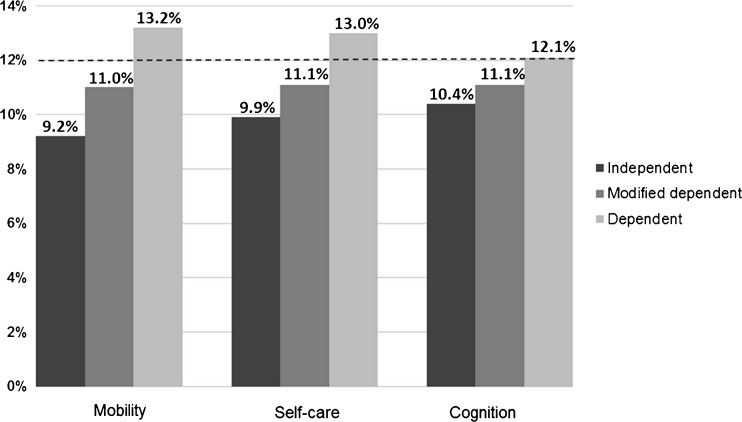
Key results: The unadjusted 30-day unplanned rehospitalization rate was 12.0 % (n = 30,179). Overall, patients dependent at discharge for mobility had a 50 % increased odds of rehospitalization (OR = 1.50, 95 % CI: 1.42-1.59), patients dependent for self-care a 36 % increased odds (OR = 1.36, 95 % CI: 1.27-1.47), and patients dependent for cognition a 19 % increased odds (OR = 1.19, 95 % CI: 1.09-1.29). Patients dependent for both self-care and mobility at discharge (n = 8312, 3.3 %) had a 16.1 % (95 % CI: 15.3-17.0 %) adjusted rehospitalization rate versus 8.5 % (95 % CI: 8.3-8.8 %) for those independent for both (n = 74,641; 29.6 %).
Conclusions: The functional domains identified in the IMPACT Act were associated with 30-day unplanned rehospitalization following post-acute care in this large national sample. Further research is needed to better understand and improve the functional measures, and to determine if their association with rehospitalizations varies across post-acute settings, patient populations, or episodes of care.
Keywords: functional status; health care reform; health services research; medicare; rehabilitation.
Conflict of interest statement
Compliance with Ethical Standards Funders The study was supported by the National Institutes of Health (R24-HD065702, R01-HD069443 and 5K12HD055929-09, PI, K. Ottenbacher) and the National Institute for Disability, Independent Living, and Rehabilitation Research (H133G140127, PI, K. Ottenbacher). Conflict of Interest The authors declare no conflicts of interest.
Figures


Comment in
-
And Now Post-Post-Acute Care Transitions.J Gen Intern Med. 2016 Dec;31(12):1410-1411. doi: 10.1007/s11606-016-3770-7. J Gen Intern Med. 2016. PMID: 27312094 Free PMC article. No abstract available.
References
-
- Deutsch A, Kline T, Kelleher C, et al. Analysis of Crosscutting Medicare Functional Status Quality Metrics Using the Continuity and Assessment Record and Evaluation (CARE) Item Set- Final Report. RTI International Report;2012.
-
- Improving Medicare Post-Acute Care Transformation Act of 2014. S. 2553. 2D ed2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
