

Intrauterine Growth Restriction: Antenatal and Postnatal Aspects
- PMID: 27441006
- PMCID: PMC4946587
- DOI: 10.4137/CMPed.S40070
Intrauterine Growth Restriction: Antenatal and Postnatal Aspects
Abstract
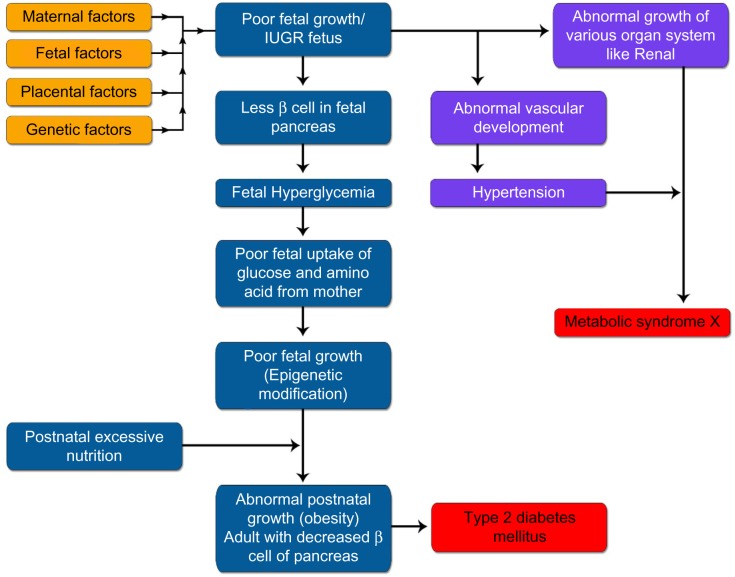
Intrauterine growth restriction (IUGR), a condition that occurs due to various reasons, is an important cause of fetal and neonatal morbidity and mortality. It has been defined as a rate of fetal growth that is less than normal in light of the growth potential of that specific infant. Usually, IUGR and small for gestational age (SGA) are used interchangeably in literature, even though there exist minute differences between them. SGA has been defined as having birth weight less than two standard deviations below the mean or less than the 10th percentile of a population-specific birth weight for specific gestational age. These infants have many acute neonatal problems that include perinatal asphyxia, hypothermia, hypoglycemia, and polycythemia. The likely long-term complications that are prone to develop when IUGR infants grow up includes growth retardation, major and subtle neurodevelopmental handicaps, and developmental origin of health and disease. In this review, we have covered various antenatal and postnatal aspects of IUGR.
Keywords: Intrauterine growth restriction (IUGR); asymmetrical IUGR; developmental origin of health and disease; fetal genes; maternal genes; placental genes; small for gestational age (SGA); symmetrical IUGR; thrifty phenotype (Barker hypothesis).
Figures









References
-
- Battaglia FC, Lubchenco LO. A practical classification of newborn infants by weight and gestational age. J Pediatr. 1967;71(2):159–63. - PubMed
-
- Sharma D, Shastri S, Farahbakhsh N, Sharma P. Intrauterine growth restriction–part 1. J Matern Fetal Neonatal Med. 2016;7:1–11.
-
- Sharma D, Farahbakhsh N, Shastri S, Sharma P. Intrauterine growth restriction – part 2. J Matern Fetal Neonatal Med. 2016;0(0):1–12.
-
- de Onis M, Blössner M, Villar J. Levels and patterns of intrauterine growth retardation in developing countries. Eur J Clin Nutr. 1998;52(Suppl 1):S5–15. - PubMed
-
- Lee PA, Chernausek SD, Hokken-Koelega ACS, Czernichow P, International Small for Gestational Age Advisory Board International Small for Gestational Age Advisory Board consensus development conference statement: management of short children born small for gestational age, April 24-October 1, 2001. Pediatrics. 2003;111(6 pt 1):1253–61. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
