

Stereotactic Ablative Radiation Therapy Combined With Immunotherapy for Solid Tumors
- PMID: 27441745
- PMCID: PMC5812885
- DOI: 10.1097/PPO.0000000000000210
Stereotactic Ablative Radiation Therapy Combined With Immunotherapy for Solid Tumors
Abstract
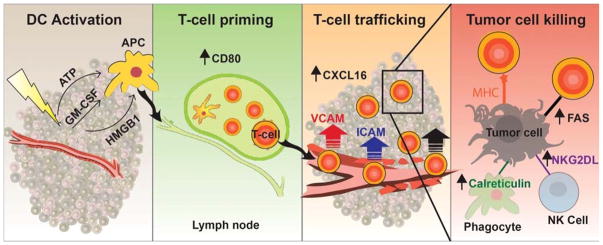
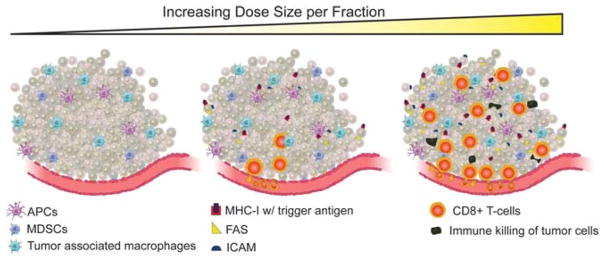
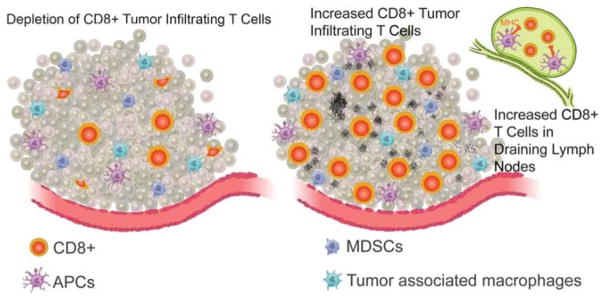
Immunotherapy, particularly immune-checkpoint inhibition, is producing encouraging clinical responses and affecting the way numerous cancers are treated. Yet immune-checkpoint therapy is not effective for many patients, and even those who initially respond can experience relapse, fueling interest in finding new processes or tools to improve the effectiveness of these novel therapeutics. One such tool is radiation. Both preclinical and clinical studies have demonstrated that the systemic effects of immunotherapy can be amplified when it is used in combination with radiation and, conversely, that the immunogenic effects of local irradiation can be amplified and extended to distant sites when used with immunotherapy. We review how stereotactic ablative radiation therapy, a technique specifically indicated for tumors treated with immune-checkpoint inhibitors, can potentiate the effects of immune-checkpoint therapy. We further explore how these novel therapeutics may transform radiation, previously considered a local treatment option, into powerful systemic therapy.
Conflict of interest statement
The authors have disclosed that they have no significant relationships with, or financial interest in, any commercial companies pertaining to this article.
Figures
References
-
- Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunity by CTLA-4 blockade. Science. 1996;271:1734–1736. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
