

Use of imaging tests after primary treatment of thyroid cancer in the United States: population based retrospective cohort study evaluating death and recurrence
- PMID: 27443325
- PMCID: PMC4955794
- DOI: 10.1136/bmj.i3839
Use of imaging tests after primary treatment of thyroid cancer in the United States: population based retrospective cohort study evaluating death and recurrence
Abstract
Objective: To determine whether the use of imaging tests after primary treatment of differentiated thyroid cancer is associated with more treatment for recurrence and fewer deaths from the disease.
Design: Population based retrospective cohort study.
Setting: Surveillance Epidemiology and End Results-Medicare database in the United States.
Participants: 28 220 patients diagnosed with differentiated thyroid cancer between 1998 and 2011. The study cohort was followed up to 2013, with a median follow-up of 69 months.
Main outcome measures: Treatment for recurrence of differentiated thyroid cancer (additional neck surgery, additional radioactive iodine treatment, or radiotherapy), and deaths due to differentiated thyroid cancer. We conducted propensity score analyses to assess the relation between imaging (neck ultrasound, radioiodine scanning, or positron emission tomography (PET) scanning) and treatment for recurrence (logistic model) and death (Cox proportional hazards model).
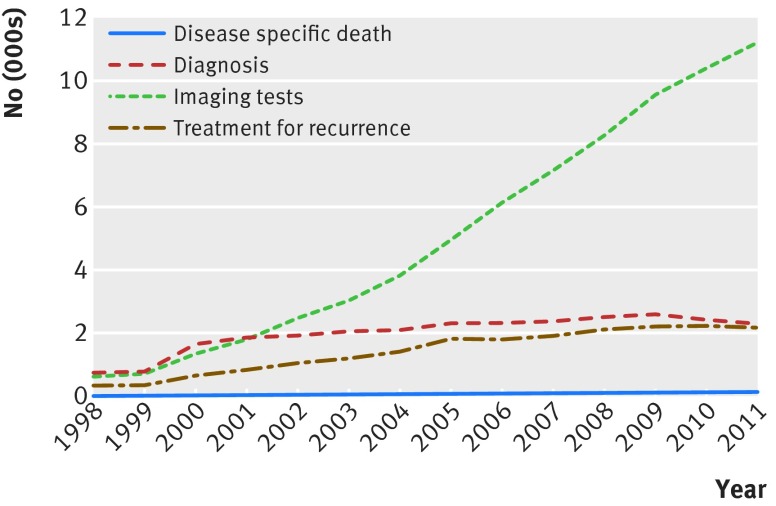
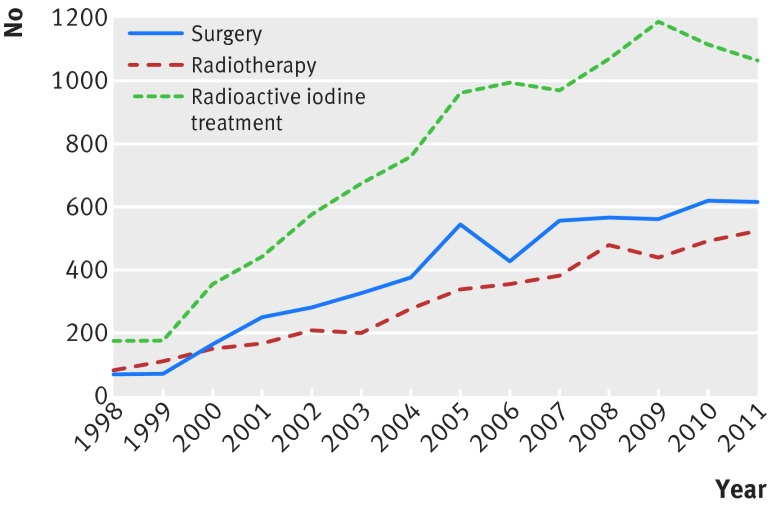
Results: From 1998 until 2011, we saw an increase in incident cancer (rate ratio 1.05, 95% confidence interval 1.05 to 1.06), imaging (1.13, 1.12 to 1.13), and treatment for recurrence (1.01, 1.01 to 1.02); the change in death rate was not significant. In multivariable analysis, use of neck ultrasounds increased the likelihood of additional surgery (odds ratio 2.30, 95% confidence interval 2.05 to 2.58) and additional radioactive iodine treatment (1.45, 1.26 to 1.69). Radioiodine scans were associated with additional surgery (odds ratio 3.39, 95% confidence interval 3.06 to 3.76), additional radioactive iodine treatment (17.83, 14.49 to 22.16), and radiotherapy (1.89, 1.71 to 2.10). Use of PET scans was associated with additional surgery (odds ratio 2.31, 95% confidence interval 2.09 to 2.55), additional radioactive iodine treatment (2.13, 1.89 to 2.40), and radiotherapy (4.98, 4.52 to 5.49). Use of neck ultrasounds or PET scans did not significantly affect disease specific survival (hazard ratio 1.14, 95% confidence interval 0.98 to 1.27, and 0.91, 0.77 to 1.07, respectively). However, radioiodine scans were associated with an improved disease specific survival (hazard ratio 0.70, 95% confidence interval 0.60 to 0.82).
Conclusions: The marked rise in use of imaging tests after primary treatment of differentiated thyroid cancer has been associated with an increased treatment for recurrence. However, with the exception of radioiodine scans in presumed iodine avid disease, this association has shown no clear improvement in disease specific survival. These findings emphasize the importance of curbing unnecessary imaging and tailoring imaging after primary treatment to patient risk.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Thyroid cancer: Mortality unaffected by rise in use of imaging tests.Nat Rev Endocrinol. 2016 Oct;12(10):560. doi: 10.1038/nrendo.2016.131. Epub 2016 Aug 5. Nat Rev Endocrinol. 2016. PMID: 27494390 No abstract available.
Similar articles
-
Neck Sonography and Suppressed Thyroglobulin Have High Sensitivity for Identifying Recurrent/Persistent Disease in Patients With Low-risk Thyroid Cancer Treated With Total Thyroidectomy and Radioactive Iodine Ablation, Making Stimulated Thyroglobulin Unnecessary.J Ultrasound Med. 2017 Nov;36(11):2299-2307. doi: 10.1002/jum.14260. Epub 2017 May 24. J Ultrasound Med. 2017. PMID: 28543974
-
Frequent screening with serial neck ultrasound is more likely to identify false-positive abnormalities than clinically significant disease in the surveillance of intermediate risk papillary thyroid cancer patients without suspicious findings on follow-up ultrasound evaluation.J Clin Endocrinol Metab. 2015 Apr;100(4):1561-7. doi: 10.1210/jc.2014-3651. Epub 2015 Jan 29. J Clin Endocrinol Metab. 2015. PMID: 25632970 Free PMC article.
-
Management and outcome of recurrent well-differentiated thyroid carcinoma.Arch Otolaryngol Head Neck Surg. 2004 Jul;130(7):819-24. doi: 10.1001/archotol.130.7.819. Arch Otolaryngol Head Neck Surg. 2004. PMID: 15262757
-
Respective roles of thyroglobulin, radioiodine imaging, and positron emission tomography in the assessment of thyroid cancer.Semin Nucl Med. 2006 Jul;36(3):194-205. doi: 10.1053/j.semnuclmed.2006.03.002. Semin Nucl Med. 2006. PMID: 16762610 Review.
-
131I therapy for pediatric thyroid cancer.Semin Pediatr Surg. 1997 Aug;6(3):128-33. Semin Pediatr Surg. 1997. PMID: 9263334 Review.
Cited by
-
Routine thyroglobulin, neck ultrasound and physical examination in the routine follow up of patients with differentiated thyroid cancer-Where is the evidence?Endocrine. 2018 Oct;62(1):26-33. doi: 10.1007/s12020-018-1720-3. Epub 2018 Aug 20. Endocrine. 2018. PMID: 30128957 Free PMC article. Review.
-
Endocrinology practice patterns of hypothyroidism and osteoporosis management in a U.S. tertiary academic medical center.Clin Diabetes Endocrinol. 2019 Jul 18;5:10. doi: 10.1186/s40842-019-0085-8. eCollection 2019. Clin Diabetes Endocrinol. 2019. PMID: 31360539 Free PMC article.
-
Ultrasonography surveillance in papillary thyroid carcinoma patients after total thyroidectomy according to dynamic risk stratification.Endocrine. 2020 Aug;69(2):347-357. doi: 10.1007/s12020-020-02347-9. Epub 2020 May 24. Endocrine. 2020. PMID: 32449109
-
Impact of periodic neck ultrasonography on locoregional disease control in surveillance after total thyroidectomy for patients with low- and intermediate-risk papillary thyroid carcinoma: a propensity score-matched study.Endocr J. 2024 Dec 2;71(12):1135-1143. doi: 10.1507/endocrj.EJ24-0194. Epub 2024 Oct 1. Endocr J. 2024. PMID: 39358211 Free PMC article.
-
Use of Neck Ultrasound as Surveillance in Older Adults With Thyroid Cancer.Endocr Pract. 2025 Aug;31(8):1033-1037. doi: 10.1016/j.eprac.2025.04.020. Epub 2025 Apr 30. Endocr Pract. 2025. PMID: 40316140
References
-
- Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg 2014;140:317-22. 10.1001/jamaoto.2014.1 pmid:24557566. - DOI - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913-21. 10.1158/0008-5472.CAN-14-0155 pmid:24840647. - DOI - PubMed
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 2006;295:2164-7. 10.1001/jama.295.18.2164 pmid:16684987. - DOI - PubMed
-
- Sprague BL, Warren Andersen S, Trentham-Dietz A. Thyroid cancer incidence and socioeconomic indicators of health care access. Cancer Causes Control 2008;19:585-93. 10.1007/s10552-008-9122-0 pmid:18240001. - DOI - PubMed
-
- Banerjee M, Muenz DG, Chang JT, Papaleontiou M, Haymart MR. Tree-based model for thyroid cancer prognostication. J Clin Endocrinol Metab 2014;99:3737-45. 10.1210/jc.2014-2197 pmid:25033070. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical