

Surgeon specialization and operative mortality in United States: retrospective analysis
- PMID: 27444190
- PMCID: PMC4957587
- DOI: 10.1136/bmj.i3571
Surgeon specialization and operative mortality in United States: retrospective analysis
Abstract
Objective: To measure the association between a surgeon's degree of specialization in a specific procedure and patient mortality.
Design: Retrospective analysis of Medicare data.
Setting: US patients aged 66 or older enrolled in traditional fee for service Medicare.
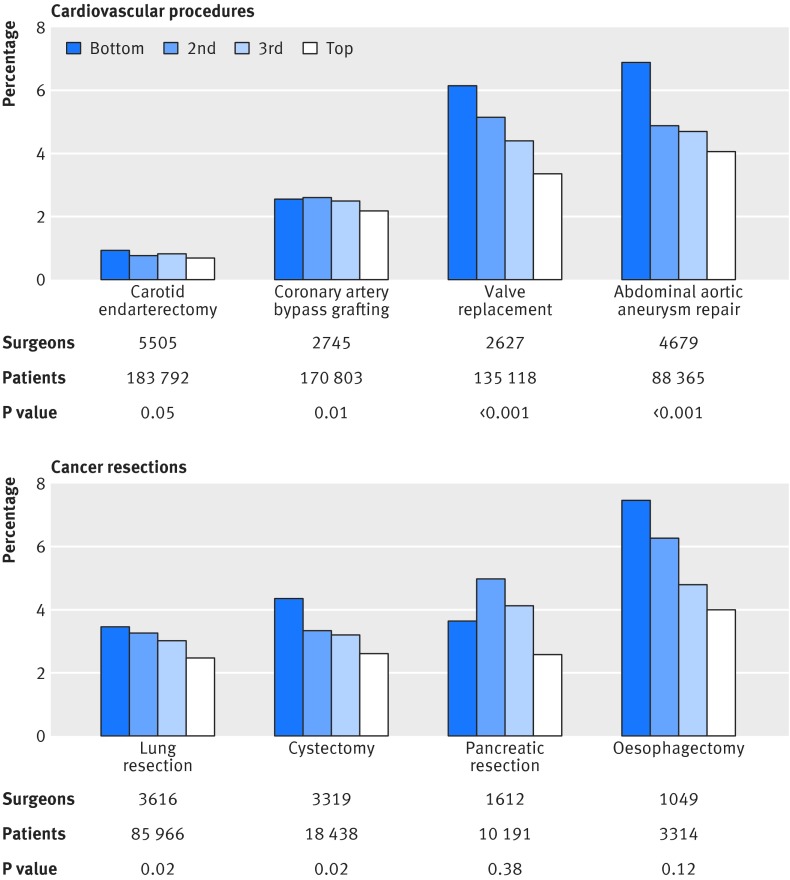
Participants: 25 152 US surgeons who performed one of eight procedures (carotid endarterectomy, coronary artery bypass grafting, valve replacement, abdominal aortic aneurysm repair, lung resection, cystectomy, pancreatic resection, or esophagectomy) on 695 987 patients in 2008-13.
Main outcome measure: Relative risk reduction in risk adjusted and volume adjusted 30 day operative mortality between surgeons in the bottom quarter and top quarter of surgeon specialization (defined as the number of times the surgeon performed the specific procedure divided by his/her total operative volume across all procedures).
Results: For all four cardiovascular procedures and two out of four cancer resections, a surgeon's degree of specialization was a significant predictor of operative mortality independent of the number of times he or she performed that procedure: carotid endarterectomy (relative risk reduction between bottom and top quarter of surgeons 28%, 95% confidence interval 0% to 48%); coronary artery bypass grafting (15%, 4% to 25%); valve replacement (46%, 37% to 53%); abdominal aortic aneurysm repair (42%, 29% to 53%); lung resection (28%, 5% to 46%); and cystectomy (41%, 8% to 63%). In five procedures (carotid endarterectomy, valve replacement, lung resection, cystectomy, and esophagectomy), the relative risk reduction from surgeon specialization was greater than that from surgeon volume for that specific procedure. Furthermore, surgeon specialization accounted for 9% (coronary artery bypass grafting) to 100% (cystectomy) of the relative risk reduction otherwise attributable to volume in that specific procedure.
Conclusion: For several common procedures, surgeon specialization was an important predictor of operative mortality independent of volume in that specific procedure. When selecting a surgeon, patients, referring physicians, and administrators assigning operative workload may want to consider a surgeon's procedure specific volume as well as the degree to which a surgeon specializes in that procedure.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Surgical training must ensure continued production of specialist surgeons.BMJ. 2016 Sep 6;354:i4702. doi: 10.1136/bmj.i4702. BMJ. 2016. PMID: 27601033 No abstract available.
References
-
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med 2003;349:2117-27. 10.1056/NEJMsa035205 pmid:14645640. - DOI - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med 2002;346:1128-37. 10.1056/NEJMsa012337 pmid:11948273. - DOI - PubMed
-
- Reames BN, Ghaferi AA, Birkmeyer JD, Dimick JB. Hospital volume and operative mortality in the modern era. Ann Surg 2014;260:244-51. 10.1097/SLA.0000000000000375 pmid:24368634. - DOI - PMC - PubMed
-
- Finks JF, Osborne NH, Birkmeyer JD. Trends in hospital volume and operative mortality for high-risk surgery. N Engl J Med 2011;364:2128-37. 10.1056/NEJMsa1010705 pmid:21631325. - DOI - PMC - PubMed
-
- Elixhauser A, Steiner C, Fraser I. Volume thresholds and hospital characteristics in the United States. Health Aff (Millwood) 2003;22:167-77. 10.1377/hlthaff.22.2.167 pmid:12674419. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical