

Complementary roles of open and hybrid approaches to thoracoabdominal aortic aneurysm repair
- PMID: 27444368
- PMCID: PMC5441846
- DOI: 10.1016/j.jvs.2016.04.022
Complementary roles of open and hybrid approaches to thoracoabdominal aortic aneurysm repair
Abstract
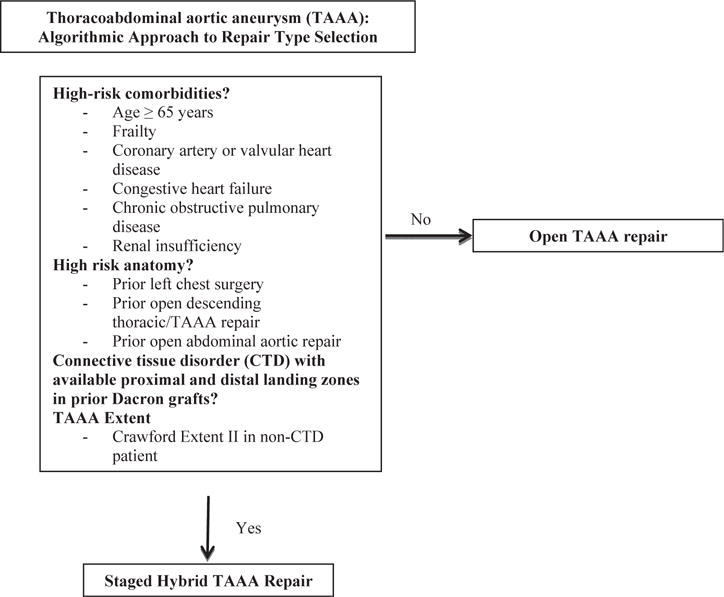
Objective: Thoracoabdominal aortic aneurysm (TAAA) repair remains a significant challenge with considerable perioperative morbidity and mortality. A hybrid approach utilizing visceral debranching with endovascular aneurysm exclusion has been used to treat high-risk patients and therefore allow repair in more patients. Limited data exist regarding long-term outcomes with this procedure as well as comparison to conventional open repair. This study describes our institutional algorithmic approach to TAAA repair using both open and hybrid techniques.
Methods: Hybrid and open TAAA repairs performed between July 2005 and August 2015 were identified from a prospectively maintained institutional aortic surgery database. Perioperative morbidity and mortality, freedom from reintervention, and long-term and aorta-specific survival were calculated and compared between the two groups.
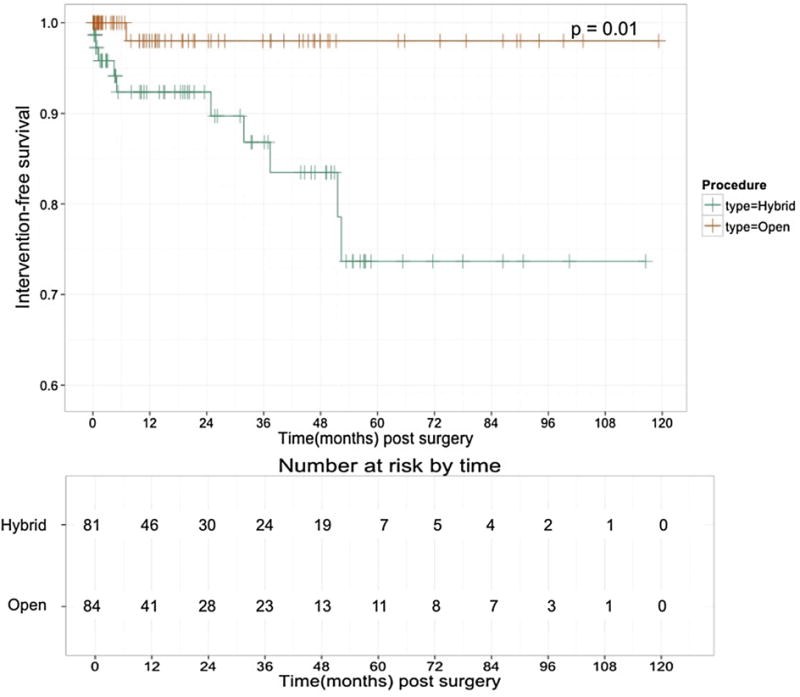
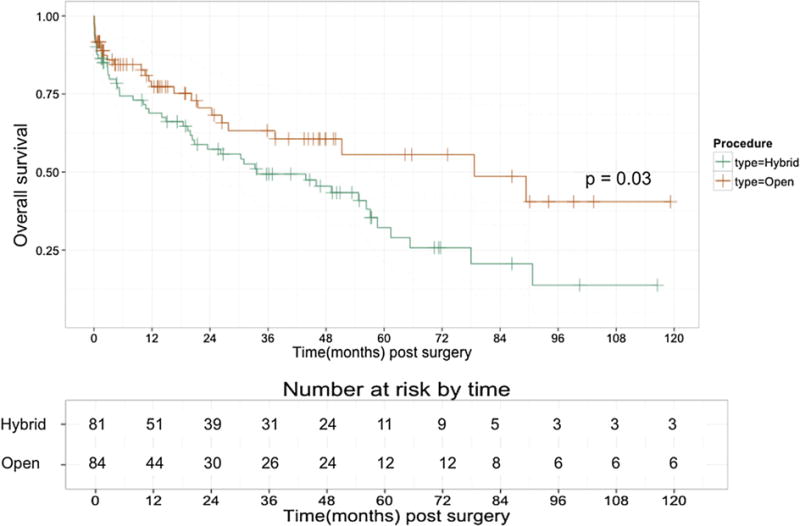
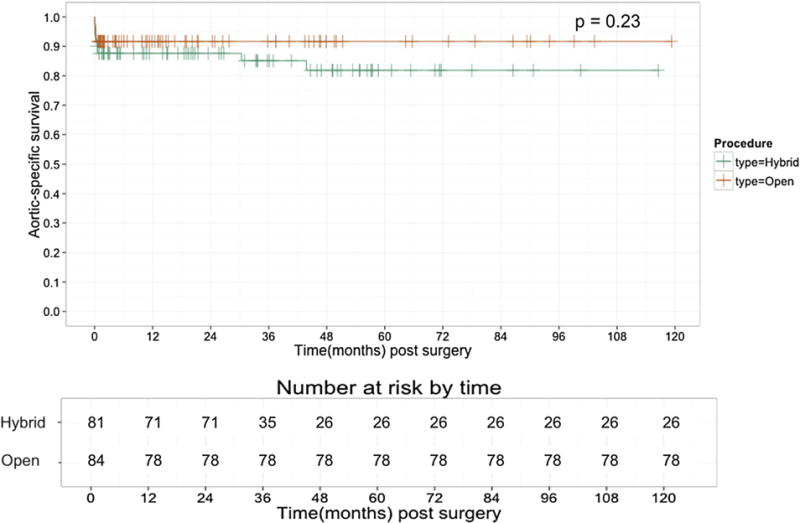
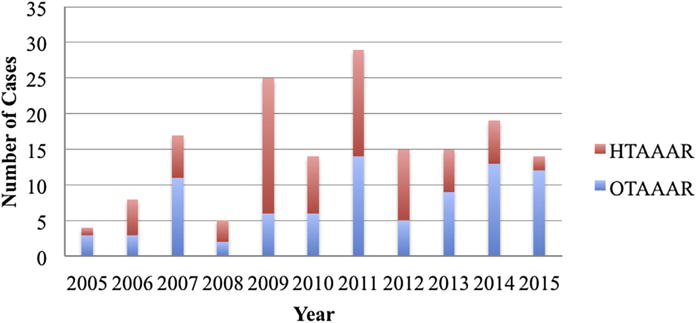
Results: During the study period, 165 consecutive TAAA repairs were performed, including 84 open repairs and 81 hybrid repairs. Patients in the hybrid repair group were significantly older, were more frequently female, and had a generally greater comorbid disease burden, including significantly more chronic kidney disease. Despite the older and sicker cohort, there was no difference in in-hospital mortality between the two groups (9.9% hybrid vs 7.1% open; P = .59). Major morbidity rates differed by procedure, with patients undergoing open repair having a significantly higher rate of postoperative stroke (9.5% open vs 0% hybrid; P = .017), whereas patients undergoing hybrid repair had a higher rate of new permanent dialysis (14.8% hybrid vs 3.6% open; P = .043). There was no difference between groups in the rate of postoperative permanent paraplegia/paresis (8.3% open vs 7.4% hybrid; P = .294). There was a significantly increased rate of reintervention in the hybrid repair group (12.3% hybrid vs 1.2% open, P = .004), with all hybrid reinterventions performed because of endoleak. One-year survival was similar between groups at 69% in hybrid repairs vs 77% in open repairs. Long-term survival was worse in the hybrid group (5-year survival, 32% hybrid vs 56% open), although late survival appeared to be influenced mainly by comorbid disease burden, given the similar long-term aorta-specific survival between groups.
Conclusions: Use of an algorithmic approach whereby higher risk patients with TAAA are treated by a hybrid approach and lower risk patients with conventional open repair yields satisfactory short- and long-term outcomes. The availability of multiple options for TAAA repair within a single center likely allows repair in more patients with consequent decrease in the risk of aorta-related death, at the expense of increased reinterventions for endoleak.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: G.C.H. has received a consulting fee from and is on the speakers bureau for W. L. Gore & Associates. He is on the speakers bureau for Vascutek, Inc.
The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
Comment in
-
Discussion.J Vasc Surg. 2016 Nov;64(5):1238. doi: 10.1016/j.jvs.2016.04.027. Epub 2016 Jul 18. J Vasc Surg. 2016. PMID: 27444367 No abstract available.
References
-
- Wong DR, Parenti JL, Green SY, Chowdhary V, Liao JM, Zarda S, et al. Open repair of thoracoabdominal aortic aneurysm in the modern surgical era: contemporary outcomes in 509 patients. J Am Coll Surg. 2011;212:569–79. discussion: 579–81. - PubMed
-
- Coselli JS, LeMaire SA, Koksoy C, Schmittling ZC, Curling PE. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm repair: results of a randomized clinical trial. J Vasc Surg. 2002;35:631–9. - PubMed
-
- Kulik A, Castner CF, Kouchoukos NT. Outcomes after thoracoabdominal aortic aneurysm repair with hypothermic circulatory arrest. J Thorac Cardiovasc Surg. 2011;141:953–60. - PubMed
-
- Lemaire SA, Jones MM, Conklin LD, Carter SA, Criddell MD, Wang XL, et al. Randomized comparison of cold blood and cold crystalloid renal perfusion for renal protection during thoracoabdominal aortic aneurysm repair. J Vasc Surg. 2009;49:11–9. discussion: 19. - PubMed
-
- Aftab M, Songdechakraiwut T, Green SY, Zarda S, Price MD, Nalty CC, et al. Contemporary outcomes of open thoracoabdominal aortic aneurysm repair in octogenarians. J Thorac Cardiovasc Surg. 2015;149(Suppl):S134–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
