

Long-Term Impact of Right Ventricular Pacing on Left Ventricular Systolic Function in Pacemaker Recipients With Preserved Ejection Fraction: Results From a Large Single-Center Registry
- PMID: 27444509
- PMCID: PMC5015385
- DOI: 10.1161/JAHA.116.003485
Long-Term Impact of Right Ventricular Pacing on Left Ventricular Systolic Function in Pacemaker Recipients With Preserved Ejection Fraction: Results From a Large Single-Center Registry
Abstract
Background: There is limited evidence of long-term impact of right ventricular pacing on left ventricular (LV) systolic function in pacemaker recipients with preserved LV ejection fraction (LVEF). The objective of the study was to evaluate the outcome and echocardiographic course of baseline preserved LVEF in a large cohort of pacemaker recipients with respect to pacing indication and degree of right ventricular pacing.
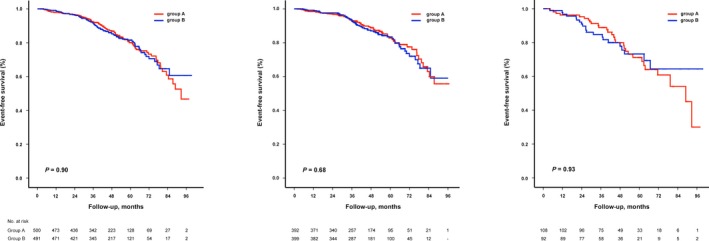
Methods and results: We enrolled 991 patients (73±10 years, 54% male) with baseline normal (>55%) LVEF (n=791) or mildly reduced (41-55%) LVEF (n=200) who had paired echocardiographic data on LV systolic function recorded at implantation and last follow-up. According to pacing indication, patients were divided into atrioventricular block group A (n=500) and sinus node disease group B (n=491). Main outcome measures were all-cause mortality and deterioration of LV function ≥2 LVEF categories at last follow-up. Patients were followed for an average of 44 months. Death from any cause occurred in 166 (17%), and deterioration of LV function ≥2 LVEF categories in 56 (6%) patients. There was no significant difference in outcome between group A and group B either in patients with normal LVEF or in those with mildly reduced LVEF. Mean percentage of right ventricular pacing was not predictive of outcome.
Conclusions: In a large cohort of pacemaker recipients with predominantly normal LVEF, clinically relevant LV dysfunction develops rather infrequently. No significant difference in all-cause mortality and development of severe LV dysfunction is observed between patients with atrioventricular block and sinus node disease. Accordingly, de novo biventricular pacing cannot be recommended for patients with preserved LVEF.
Keywords: bradycardia; cardiac resynchronization therapy; heart failure; left ventricular ejection fraction; pacemaker; right ventricular pacing; ventricular dyssynchrony.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures




References
-
- Tops LF, Schalij MJ, Holman ER, van Erven L, van der Wall EE, Bax JJ. Right ventricular pacing can induce ventricular dyssynchrony in patients with atrial fibrillation after atrioventricular node ablation. J Am Coll Cardiol. 2006;48:1642–1648. - PubMed
-
- Thambo JB, Bordachar P, Garrigue S, Lafitte S, Sanders P, Reuter S, Girardot R, Crepin D, Reant P, Roudaut R, Jais P, Haissaguerre M, Clementy J, Jimenez M. Detrimental ventricular remodeling in patients with congenital complete heart block and chronic right ventricular apical pacing. Circulation. 2004;110:3766–3772. - PubMed
-
- Tse HF, Lau CP. Long‐term effect of right ventricular pacing on myocardial perfusion and function. J Am Coll Cardiol. 1997;29:744–749. - PubMed
-
- Tops LF, Suffoletto MS, Bleeker GB, Boersma E, van der Wall EE, Gorcsan J III, Schalij MJ, Bax JJ. Speckle‐tracking radial strain reveals left ventricular dyssynchrony in patients with permanent right ventricular pacing. J Am Coll Cardiol. 2007;50:1180–1188. - PubMed
-
- Sweeney MO, Hellkamp AS. Heart failure during cardiac pacing. Circulation. 2006;113:2082–2088. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
