

Plugs of the Air Passages: A Clinicopathologic Review
- PMID: 27445091
- PMCID: PMC6026239
- DOI: 10.1016/j.chest.2016.07.003
Plugs of the Air Passages: A Clinicopathologic Review
Abstract
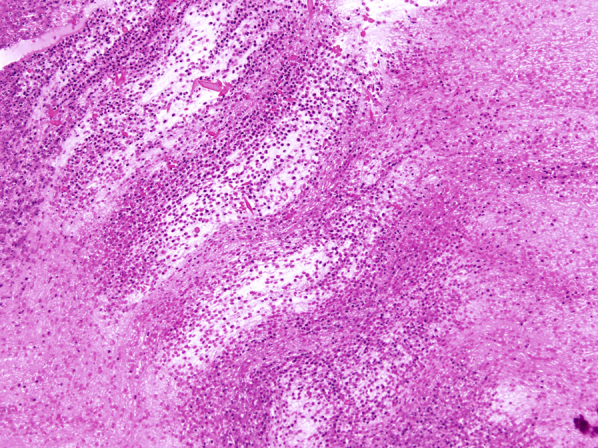
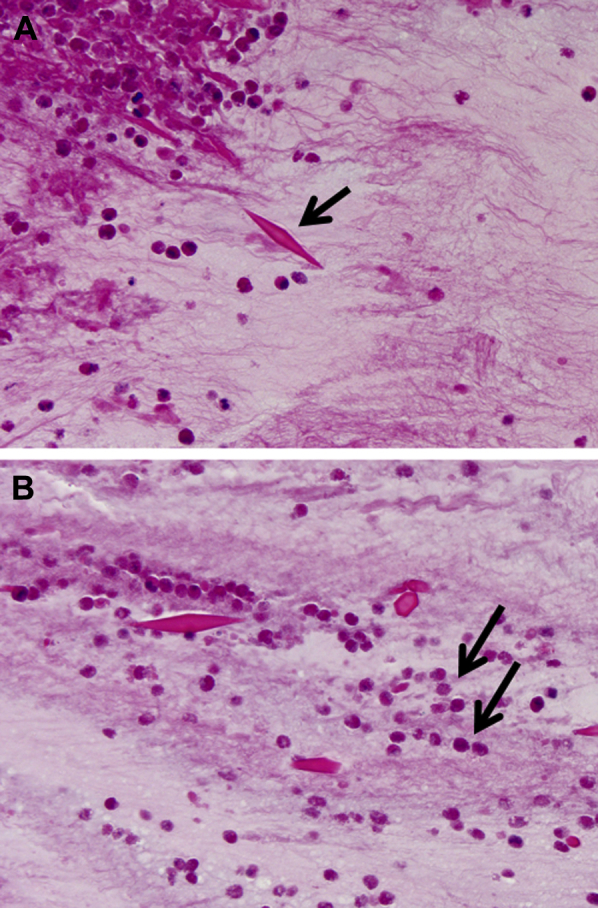
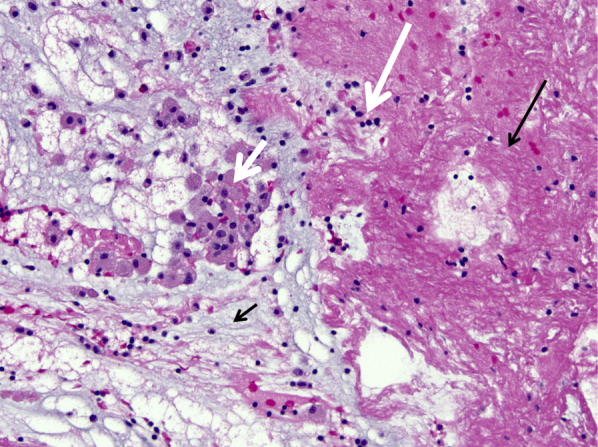
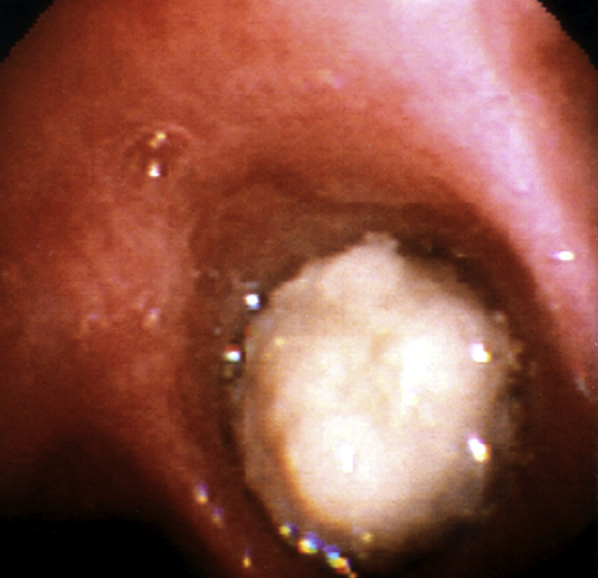
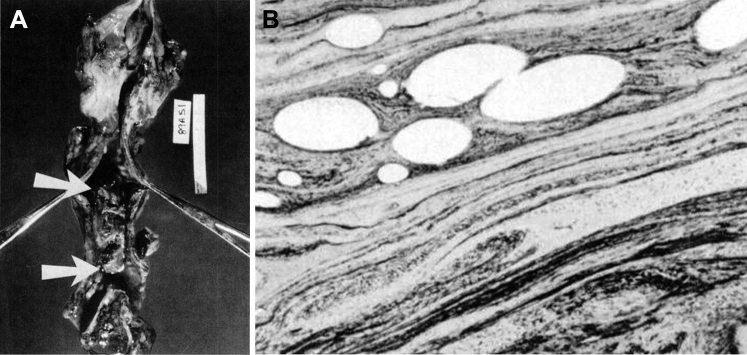
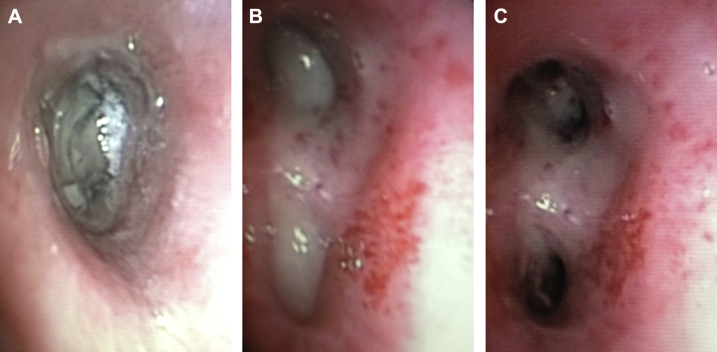
Although mucus is a normal product of the tracheobronchial tree, some diseases of the respiratory tract are characterized by unusually thick (inspissated) forms of mucus that accumulate within the airways. These are known as mucus plugs. The pathologic composition of these plugs is surprisingly diverse and, in many cases, correlates with distinctive clinical, radiologic, and bronchoscopic findings. The best-known conditions that involve mucus plugs are allergic bronchopulmonary aspergillosis, plastic bronchitis, and asthma. Other lung diseases occasionally associated with plugs within the airways include Aspergillus tracheobronchitis, hyper-IgE syndrome, exogenous lipoid pneumonia, pulmonary alveolar proteinosis, and chronic eosinophilic pneumonia. In this review, we describe and illustrate the bronchoscopic, pathologic, and imaging findings in respiratory disorders characterized by mucus plugs or plugs composed of other similar materials. Recognition of the characteristic appearance and differential diagnosis of mucus plugs will hopefully facilitate diagnosis and management of these diseases.
Keywords: airway and airspace diseases; bronchoscopic appearance; bronchoscopy; mucoid pseudotumor; mucus plugging.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Rose M.C., Voynow J.A. Respiratory tract mucin genes and mucin glycoproteins in health and disease. Physiol Rev. 2006;86(1):245–278. - PubMed
-
- Karasick D., Karasick S., Lally J.F. Mucoid pseudotumors of the tracheobronchial tree in two cases. AJR Am J Roentgenol. 1979;132(3):459–460. - PubMed
-
- Bosken C.H., Myers J.L., Greenberger P.A., Katzenstein A.L. Pathologic features of allergic bronchopulmonary aspergillosis. Am J Surg Pathol. 1988;12(3):216–222. - PubMed
-
- Mukhopadhyay S., Gal A.A. Granulomatous lung disease: an approach to the differential diagnosis. Arch Pathol Lab Med. 2010;134(5):667–690. - PubMed
-
- Katzenstein A.L., Liebow A.A., Friedman P.J. Bronchocentric granulomatosis, mucoid impaction, and hypersensitivity reactions to fungi. Am Rev Respir Dis. 1975;111(4):497–537. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
