

Renal Survival in Patients with Collapsing Compared with Not Otherwise Specified FSGS
- PMID: 27445167
- PMCID: PMC5053801
- DOI: 10.2215/CJN.13091215
Renal Survival in Patients with Collapsing Compared with Not Otherwise Specified FSGS
Abstract
Background and objectives: Idiopathic collapsing FSGS has historically been associated with poor renal outcomes. Minimal clinical data exist on the efficacy of immunosuppressive therapy. Our study sought to provide a comprehensive description of renal survival in patients with collapsing and not otherwise specified FSGS after controlling for factors affecting renal prognosis.
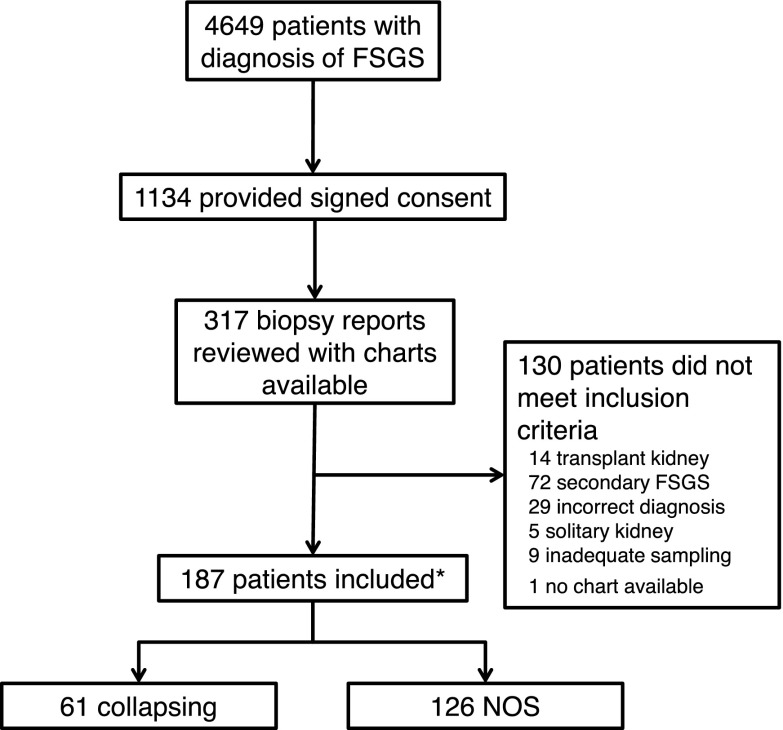
Design, setting, participants, & measurements: We performed a retrospective analysis of an inception cohort study of patients diagnosed between 1989 and 2012. All potential patients with collapsing FSGS fulfilling the inclusion criteria were identified and compared with patients with not otherwise specified FSGS (approximately 1:2 ratio) on the basis of biopsy report and record availability. Time to ESRD was analyzed using Cox proportional hazards models.
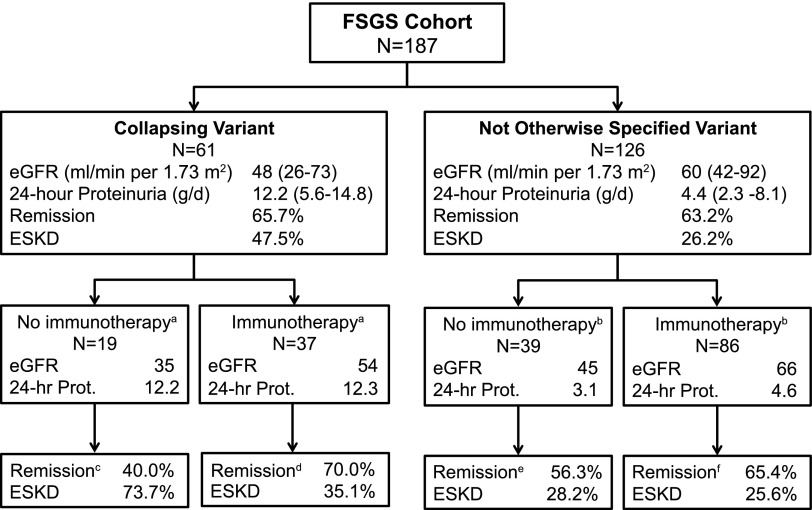
Results: In total, 187 patients were studied (61 collapsing and 126 not otherwise specified), with a mean follow-up of 96 months. At baseline, patients with collapsing FSGS had higher median proteinuria (12.2 [5.6-14.8] versus 4.4 [2.3-8.1] g/d, respectively; P<0.001), lower median albuminemia (2.4 [1.9-3.0] versus 2.9 [1.8-3.7] g/dl, respectively; P=0.12), and lower median eGFR (48 [26-73] versus 60 [42-92] ml/min per 1.73 m2, respectively; P=0.01) than patients with not otherwise specified FSGS. The proportion of patients with remission of proteinuria was similar in patients with collapsing FSGS and patients with not otherwise specified FSGS (65.7% [23 of 35] versus 63.2% [72 of 114], respectively; P=0.84). The overall renal outcome (ESRD defined as eGFR<15 ml/min per 1.73 m2, dialysis, or transplantation) of patients with collapsing FSGS was not poorer than that of patients with not otherwise specified FSGS in multivariate analyses after adjusting for baseline characteristics and immunotherapy (hazard ratio, 1.78; 95% confidence interval, 0.92 to 3.45).
Conclusions: Compared with not otherwise specified FSGS, idiopathic collapsing FSGS presented with more severe nephrotic syndrome and lower eGFR but had a similar renal survival after controlling for exposure to immunosuppressive treatment. These results highlight the importance of early diagnosis and institution of immunosuppressive therapy in patients with collapsing FSGS.
Keywords: Follow-Up Studies; Humans; Kidney Failure, Chronic; Prognosis; Proportional Hazards Models; focal segmental glomerulosclerosis; glomerular filtration rate; glomerulonephritis; immunosuppression; nephrotic syndrome; proteinuria; renal dialysis.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Haas M, Meehan SM, Karrison TG, Spargo BH: Changing etiologies of unexplained adult nephrotic syndrome: A comparison of renal biopsy findings from 1976-1979 and 1995-1997. Am J Kidney Dis 30: 621–631, 1997 - PubMed
-
- Kitiyakara C, Eggers P, Kopp JB: Twenty-one-year trend in ESRD due to focal segmental glomerulosclerosis in the United States. Am J Kidney Dis 44: 815–825, 2004 - PubMed
-
- D’Agati VD, Kaskel FJ, Falk RJ: Focal segmental glomerulosclerosis. N Engl J Med 365: 2398–2411, 2011 - PubMed
-
- Detwiler RK, Falk RJ, Hogan SL, Jennette JC: Collapsing glomerulopathy: A clinically and pathologically distinct variant of focal segmental glomerulosclerosis. Kidney Int 45: 1416–1424, 1994 - PubMed
-
- Korbet SM: Treatment of primary FSGS in adults. J Am Soc Nephrol 23: 1769–1776, 2012 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
